In 2007, I asked a dermatologist if low blood flow or poor circulation causes hair loss. He answered with a firm no. He told me that when he cuts into a balding scalp, it bleeds… a lot. He mentioned that the scalp is one of the most densely vascularized regions in the entire body — and as such, there’s just no way a restricted blood supply could cause androgenic alopecia (or pattern hair loss).
At first, I accepted the argument. After all, scalp tissues do have a dense capillary network. Accordingly, scalps have about ten times the blood flow of other anatomical regions. Scalps also bleed excessively during surgery… yet men and women still lose hair there.
So, maybe poor circulation or low blood flow doesn’t cause androgenic alopecia (AGA).
But at the same time, a lot of evidence contradicts with this statement.
For instance, hair requires blood, oxygen, and nutrients to grow. And this study revealed that balding scalps have 40% less oxygen than non-balding scalps. Blood carries oxygen, so presumably, balding scalp tissues also have lower blood flow…
And they do! This study demonstrated that compared to non-balding scalps, balding scalps have 2.6 times less subcutaneous blood flow! And if blood supply is what fuels hair growth, then it make sense that lower blood flow would lead to hair loss.
This concept isn’t new to most readers here. I’ve written about the hair loss-blood flow connection before. I’ve also published a paper touching on the topic. And in these writings, I tend to convey a pretty straightforward argument: that low blood flow does cause pattern hair loss.
But the truth is… I was oversimplifying things. The science is far more nuanced and complex than I suggested. In fact, it’s not entirely clear what role poor circulation has in AGA… if any at all.
This article explains why. And this time, no simplifications. We’re diving into the circulation-AGA connection and all its nuance. And just as a heads up — this article gets a little technical.
First, we’ll uncover a major study that led scientists to conclude that poor circulation doesn’t cause AGA. In other words, we’ll build the strongest opposition to the idea that reduced blood flow causes pattern hair loss. Then we’ll build the counterargument — revealing new findings that contradict a 50+ year-old belief about the blood flow-hair loss connection.
Finally, I’ll explain where I stand on the issue — and why, when it comes to reversing AGA, improving blood flow is incredibly hard. By the end, we should have gained a firm understanding of the hair cycle, how it influences scalp blood flow, where AGA morphology comes into play… and why these factors make it so hard to parcel out causation from correlation for poor circulation and AGA.
If you have any questions, please reach out in the comments!
Does low blood flow cause AGA? Maybe not.
The blood flow-AGA debate isn’t new. It’s as old as Roman times, with Julius Caesar reportedly believing his own male pattern baldness was due to poor scalp circulation. But it wasn’t until 1959 that investigators attempted to evaluate (in a scientific setting) whether this belief held merit.
The experiment was simple: using cadavers, researchers took biopsies of human scalp skin. Then, under a microscope, they examined the scalp skin’s hair follicles (and hair) and attempted to answer a simple question:
As a hair transitions into later stages of the hair cycle, what causes the degradation of that hair’s blood supply?
In reality, that’s not a simple question. But if we’re to understand the relationship between blood flow and pattern hair loss, we need to also understand the hair cycle… and why, when it comes to AGA pathology, answering this “simple” question is so important.
What is the hair cycle?
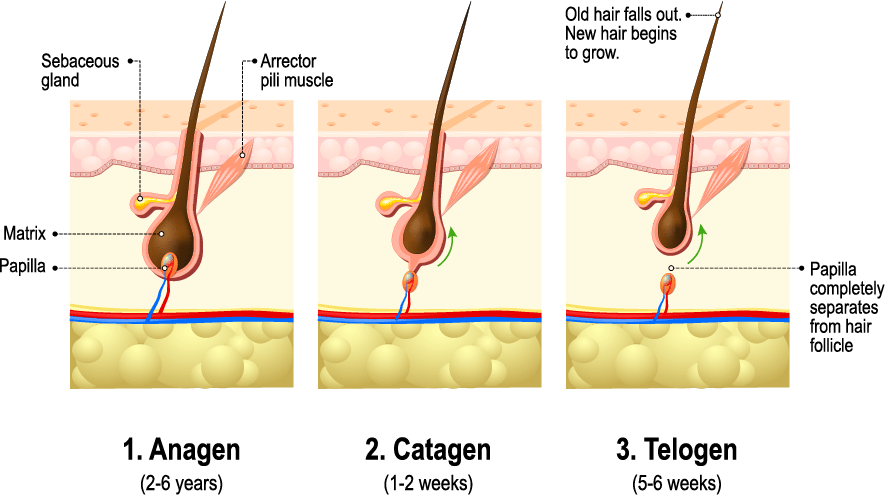
Our hairs are in a constant state of growing, shedding, or regenerating. This phenomenon is known as the hair cycle. And hair loss researchers like to think about the hair cycle in three stages: anagen (growth), catagen (resting), and telogen (shedding).
To identify the “stage” of any hair, we need to biopsy the scalp skin, look under a microscope, and answer two questions:
- Is the hair still growing?
- Is the hair still connected to its main blood supply?
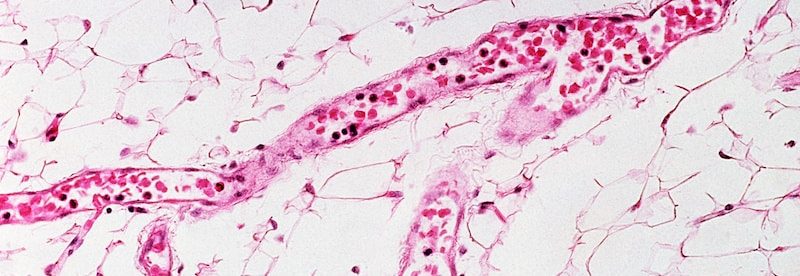
And that means we need to look at our scalp skin from this angle (i.e., a biopsy):

Note in this graphic: those blue and red lines are small microvascular networks. Those networks are the main blood supply of the hair. And that seed-like cluster at the hair base? That’s called the dermal papilla.
The dermal papilla is what connects the hair follicle to its microvascular network. It’s sort of like the hair’s powerhouse. The dermal papilla takes in energy (i.e., blood, nutrient, and oxygen from the microvascular networks) and turns that energy into hair growth. It goes without saying that in the absence of a dermal papilla, hair cannot grow.
Knowing this, we can better define the three stages of the hair cycle. After all, each hair “stage” is defined by 1) whether a hair is still growing, and 2) the connection of that hair to the dermal papilla.
- Anagen (growing) (~85% of our scalp hair). Anagen hairs are growing, and still firmly connected to the dermal papilla.
- Catagen (resting) (~1% of our scalp hair). Catagen hairs are not growing, and their dermal papilla is beginning to descend away from the hair base.
- Telogen (shedding) (~10-15% of our scalp hair). Telogen hairs are not growing and are ready to fall out at any moment. Moreover, their dermal papilla has completely detached from the hair base. With 10-15% of our scalp hair in the telogen stage, this is why we lose 100+ hairs daily (even in the absence of pattern hair loss).
Once a telogen hair sheds, the dermal papilla regenerates and forms a new anagen hair… and the cycle repeats. In fact, here’s a graphic showing all three hair cycle stages:
Again: as the hair moves from anagen to catagen, the dermal papilla shrinks and descends away from the hair base… as does the hair’s blood supply.
This is important. Why? Because as the dermal papilla and blood supply shrink, so does the amount of blood pumping to the hair follicle. That means that hairs in catagen (resting) have less blood supply than hairs in anagen (growth).
Why is this relevant to AGA?
Well, when a hair begins to miniaturize during AGA, they reach a point where they become “stuck” in a catagen- or telogen-like state. For instance, according to this review, we see…
- Reduced hair follicle size and hair length
- Reduced dermal papilla size
- Reduced / degenerating micro-capillary networks to the dermal papilla
Thus, if we want to understand the order of events in AGA (i.e., if blood flow causes pattern hair loss), we need to understand what happens first as a hair enters into categen (resting). Specifically…
Does a hair stop growing after… or before that hair’s microvascular networks degenerate?
If hair growth stops after its blood supply degenerates, this implies reduced blood supply might’ve caused the hair to stop growing. If a hair stops growing before, this suggests reduced blood flow is not the cause of hair loss, but the effect.
This is what that 1959 study attempted to answer. Hence the researchers’ question:
What causes the reduction in blood supply as a hair enters into the catagen stage of the hair cycle?
And now we can begin to uncover the answers.
Do catagen hairs stop growing before or after their blood supply degenerates?
At first, the answer seems obvious. Let’s think about it…
Micro-capillary networks supply nutrients to the dermal papilla — the “powerhouse” of a hair follicle. If the power to that powerhouse (i.e., the blood vessels) decreases, then the output of that powerhouse (i.e., hair growth) must also decrease. So we should presume the order of events is…
- Capillary networks connected to the dermal papilla begin to degenerate, thus reducing nutrient transport, blood, and oxygen supply to the dermal papilla.
- In response, the dermal papilla shrinks to compensate for lower energy intake, and starts to descend from the hair.
- Eventually, the dermal papilla detaches from the hair entirely — disconnecting the hair from its powerhouse — causing the hair to stop growing.
This is a logical, well-reasoned sequence of events. And before researching AGA and hair cycle disorders, I believed it to make sense. There’s just one issue…
It’s 100% wrong. In fact, that 1959 study proved it. Shockingly, these researchers discovered — contrary to what was expected — that a hair actually stops growing before its capillary network (i.e., blood supply) degenerates.
Hair stops growing before its blood vessels degenerate.
That’s right. According to that study, the order is actually…
- A hair stops growing, and resultantly…
- The dermal papilla and capillary networks degenerate and eventually disconnect from the hair base.
This means that scalp blood flow decreases after a hair stops growing. And it bears emphasizing: this is completely unintuitive (at least to me).
Why? Let’s go back to our powerhouse analogy. Saying that a hair stops growing before its capillary networks degenerate is like saying that a box of chocolates stopped making itself so its factory workers (the dermal papilla and blood supply) could skip work the next day. It makes no sense.
And yet this is exactly what happens in our own scalps. In fact, here’s the quote from the paper:
These observations indicate that the degeneration of the blood vessels in the dermal papilla during catagen is a secondary effect and not the primary cause for cessation of hair growth.
What’s more, these findings aren’t just one-offs. They’ve been confirmed again… and again.
Which begs the question…
If a hair stops growing before its dermal papilla and blood supply degenerate, what triggers that hair to stop growing?
Luckily, these investigators identified a few culprits. In the biopsy photos, they noticed three distinct changes in a catagen hair’s surrounding tissue that directly preceded a stop in hair growth. They were:
- Changes to the connective tissue sheath
- Changes to the glassy membrane
- Changes to the external root sheath
Don’t worry about these new terms. All we need to know is where they are. See the below graphic (in the middle-left).
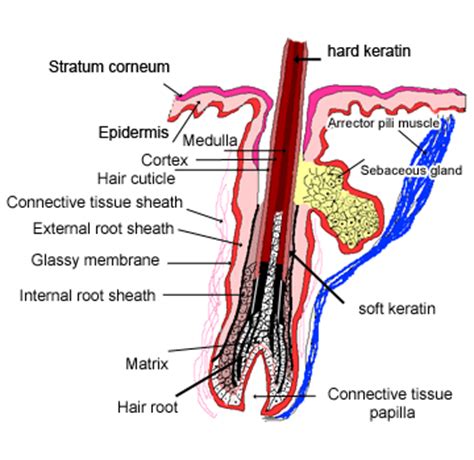
(source)
We can see the connective tissue sheath, external root sheath, and glassy membrane are all next to each other, surrounding the hair shaft. They’re known as mesodermal tissues (i.e., tissues surrounding where the hair grows).
And here’s what these investigators observed:
Right before a hair stops growing, these mesodermal tissues expand and distort. In doing so, they constrict the width of the hair shaft. This constriction pinches the hair, signaling for it to stop growing… which then signals to the dermal papilla and microvascular networks to degenerate.
Again, just to summarize the order. In the catagen phase of the hair cycle…
Mesodermal sheaths expand >> hair shaft gets pinched >> hair stops growing >> dermal papilla and blood vessels degenerate
This means that reduced blood flow comes after a hair stops growing.
And this had huge implications for AGA. Why? Because AGA-affected hairs undergo changes very similar to the ones observed in catagen (resting) and telogen (shedding) hairs. And after all, AGA-affected scalps have lower blood flow than non-balding scalps…
So… what did investigators extrapolate?
Reduced blood flow doesn’t cause AGA… AGA causes reduced blood flow.
This is why, in literature reviews, so many AGA investigators state that reduced blood flow in AGA happens after the hairs start to miniaturize. In other words, low blood flow is the effect of AGA… not the cause.
However, we’ve only built the strongest opposition to the “poor circulation causes hair loss” argument. In other words, we’re still missing the other half of the debate!
And if you haven’t already noticed, there’s one major problem with the opposition’s logic…
Hair cycling and AGA are not synonymous.
Androgenic alopecia (AGA) is characterized by the following three traits:
- Hair follicle miniaturization. In affected regions, the diameter of each hair strand gets progressively thinner.
- Increased telogen:anagen ratio. In affected regions, ratio of shedded versus growing hairs increases.
- Increased anagen cycling. In affected regions, hairs grow for shorter time periods before they cycle into resting.
Yes, the hair cycle is undoubtedly involved in this process. For instance, many researchers argue that the step-process for hair follicle miniaturization is as follows:
- A hair strand disconnects from its hair follicle base (catagen)
- The hair sheds (telogen), and the follicle degenerates (loss of blood flow)
- A new hair follicle is created where the old one once was (new anagen), but…
- That follicle has a smaller dermal papillae cluster, and thereby produces a smaller hair follicle, which produces a tinier hair strand
And again, this is why some researchers believe low blood flow is a consequence (and not a cause) of AGA. If a hair strand disconnects from its hair follicle base before that hair follicle degenerates (and thereby loses blood flow), then this would imply that the loss of blood flow is a consequence of the hair shedding… not the other way around.
This is true, but only if we maintain a myopic view of everything that happens in a balding scalp.
If we actually expand our vantage point to the entire scalp itself, it becomes clear there’s much more to discuss… and many other places where scalp blood flow is reduced.
Which brings us to our counterargument.
The evidence that reduced blood flow causes pattern hair loss
The problem with scalp biopsies
Before moving forward, it’s important to note that nearly everything we know about hair loss “histology” – i.e., what hair loss disorders look like underneath the skin – comes through research on scalp biopsies. In living subjects, these are small “punch” incisions – generally no more than 4mm x 4mm – where someone is losing their hair. Investigators will take these tissue samples, examine them under a microscope, and use the histological presentations of the sample to make a better hair loss diagnosis.
Scalp biopsies are incredibly useful tools, but they require an important caveat: they only provide a 4mm x 4mm perspective of the balding process. These biopsies create somewhat of a myopic bias in the research of hair loss pathophysiology: we’re only looking for the “cause-and-effect” of hair follicle miniaturization in the regions directly surrounding the hair follicle. This begs the question:
What if we expand our view and look at the histology of the entire scalp?
When we do this, we see that there’s another key region in which blood flow is reduced… one that might even contribute to the three defining characteristics of AGA: hair follicle miniaturization, increased telogen:anagen ratios, and increased anagen cycling.
It’s the scalp perimeter muscles.
Some evidence suggests that 80% of men with AGA have involuntarily chronically contracted scalp perimeter muscles
The blood supply for our extremities (i.e., our hands and feet) originate from one place: the heart. Our scalps are no different. And that means that the blood supplying the tops of our scalps (i.e., hair follicles) must originate from below, and must travel up.
Blood vessels develop through paths of “least resistance”. And that means that the blood vessels that support the tops of our scalps originate from below… and must pass through the muscle tissues along the perimeters of our scalps.
While researching botulinum toxin (i.e., Botox) as a treatment to relieve tension headaches, Dr. Freund noticed that his male and female patients with AGA (including himself) also had extremely tight scalp perimeter muscles.
Anatomically, when a muscle is flexed, it expands against its surrounding tissues… much like the mesodermal sheath expands against the hair shaft. And like the mesodermal expansion, chronic muscle contract also has a consequence: the pinching and compression of its blood vessel networks. Specifically, the blood vessels that supply the top parts of our scalps… the region where we suffer from pattern hair loss.
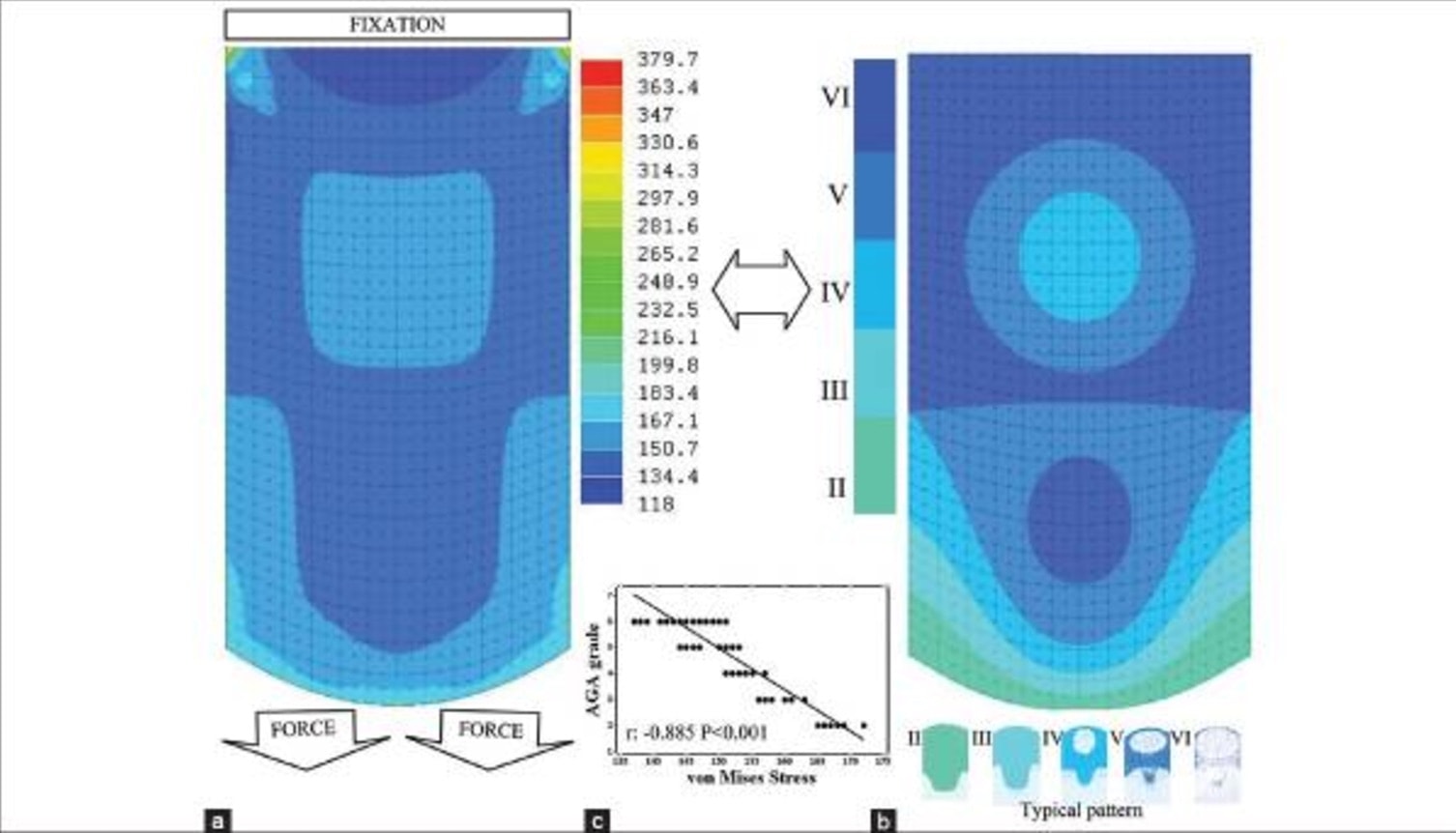
Interestingly, the investigators of this study revealed that balding scalps have 40% less transcutaneous oxygen than non-balding scalps… and postulated that the drop in oxygen levels couldn’t be due to hair cycle changes alone. And more importantly, that same study showed that when oxygen levels drop below a certain threshold, fibrosis forms… the same fibrosis we see in AGA.
Dr. Freund hypothesized that the chronic contraction of the scalp’s perimeter muscles might be the cause of this reduced blood flow. After all, this chronic muscular contraction should theoretically pinch the capillary networks which supply blood to AGA tissues, thereby constricting their flow and decreasing oxygen, blood, and nutrient levels.
So Dr. Freund set out to test his hypothesis. He injected a group of AGA-affected men with Botox – a neuro-modifier that forces muscles to relax. He made these injections into all the muscles lining the perimeter of the scalp. And six months later, when the effects began to wear off, he brought these men back in for another round of injections.
After almost a year, the men came back in to gauge their change in hair count. The results: a 75% response rate for the treatment group… and an 18% increase in hair count in less than a year.
For what it’s worth, Dr. Freund’s research has been validated again and again. And interestingly, the response rates to these studies all seem to land around 80%.
In other words, 80% of men with AGA saw hair loss improvements after taking their scalp perimeter muscles out of chronic contraction, and thereby purportedly unclamping the arterial branches running through these muscles to improve blood flow to the top of the scalp.
And what does that suggest? Two things:
- For ~80% of men with AGA, reductions in blood flow don’t just occur as a consequence of increased hair cycling and hair follicle miniaturization; they also occur because the scalp perimeter muscles might be pinching arterial passageways and thus restricting blood supply to the top of the scalp.
- For ~80% of men with AGA, relaxing these muscles improves hair growth… and at a significant magnitude.
To me, this evidence suggests that we cannot use research on the hair cycle to claim that low blood flow is a consequence of AGA, not a cause. Rather, if we expand our vantage point to the rest of the balding scalp, it’s possible that reduced blood flow might also occur as a result of the clamping of arterial branches… and that by unclamping these branches through muscle relaxants like botulinum toxin, we might improve blood flow and thereby improve AGA outcomes.
Therefore, low blood flow is probably both a cause and consequence of AGA, depending on where you’re looking. It’s a consequence directly surrounding hair follicles, and potentially, also a cause if we zoom out and look at blood flow reductions to the entire scalp from the pinching of arterial branches surrounding the scalp perimeter muscles.
Another potential contributing factor: how muscular contractions may also trigger chronic scalp tension (and chronic inflammation)
To emphasize, this is all hypothetical, and getting into the details here requires a separate article. But here are the highlights:
In 2015, this research team demonstrated that when muscles surrounding our scalp perimeter contract, they form a tension pattern at the top of our scalps that closely aligns with the pattern and progression of AGA. Here’s the model:
As we already know, chronic tension can be interpreted in the body as inflammation. And interestingly, this might have implications in AGA.
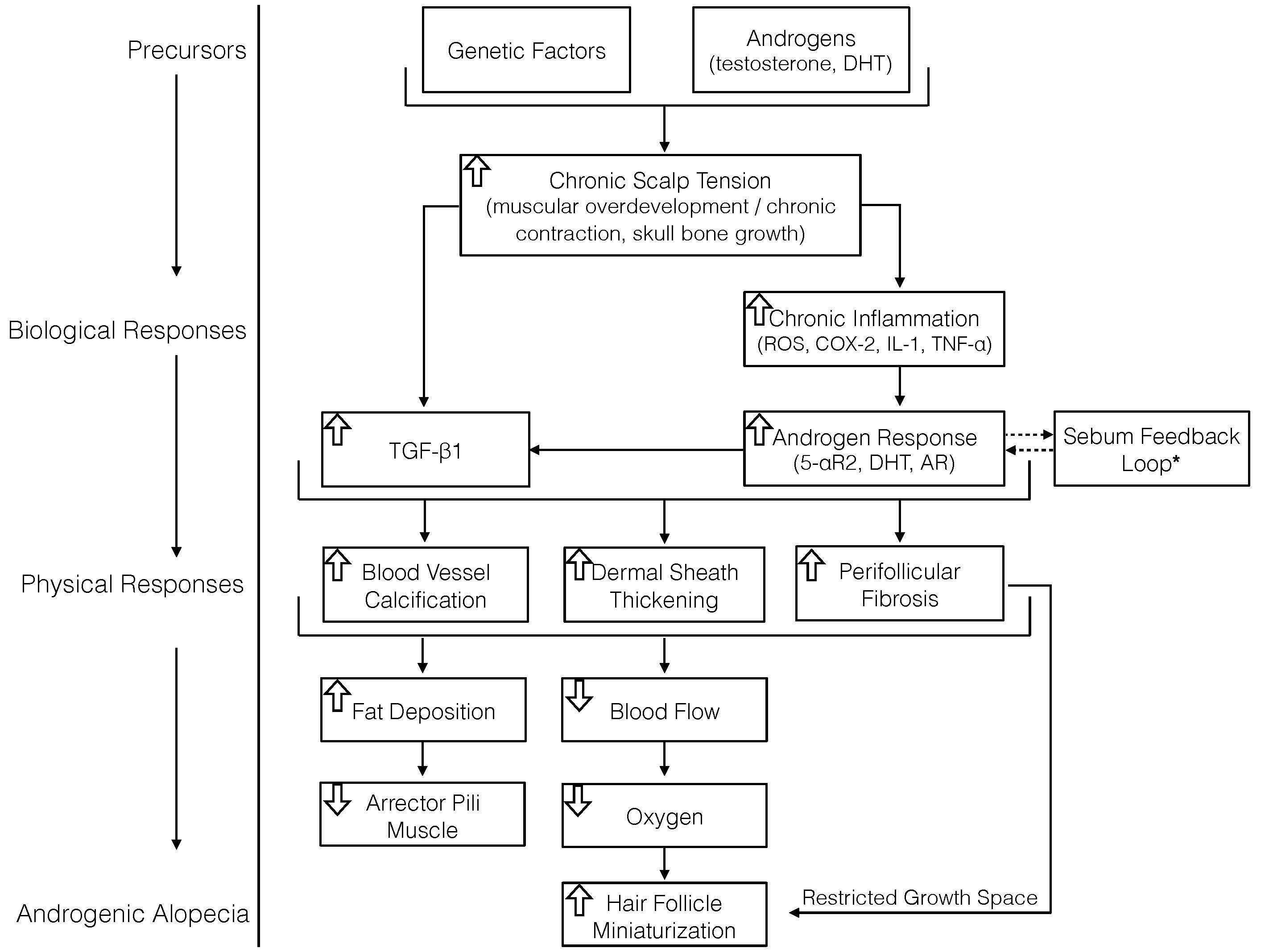
Resultantly, inflammatory models suggest that our bodies often try to “respond” to inflammation by sending signaling proteins (i.e. TGF-B1) and hormones (i.e., DHT) to resolve the insult. But if this tensile model holds true, then since inflammation in AGA would then be partly tension-derived — and not injury- or infection-derived — our bodies can’t resolve it with an inflammatory response. The end-result: a chronic, low-grade attempt at resolving inflammation that can only be resolved by relieving tension.
Eventually, this chronic inflammation would result in the accumulation of scar tissue. Specifically, fibrosis in mesodermal tissues. And just like mesodermal sheath expansion in the catagen phase of the hair cycle, any additional accumulation of tissue in these regions will constrict hair shaft space… leading to the progressive miniaturization of hair.
In this model, the order of operations looks like this:
Scalp muscles contract >> tension generates across top of scalp >> inflammatory response >> fibrosis in mesodermal sheath >> mesodermal tissue expansion >> hair shaft constriction alongside reduced blood flow >> hair loss.
This is why I believe that poor circulation might also be a cause of pattern hair loss. And this is why I still stand by the AGA pathology model I proposed in my paper:
Summary
End-stages of the hair cycle (i.e., catagen and telogen) share histological similarities with parts of AGA progression. Resultantly, some investigators use histological studies on the hair cycle to try and explain the order of events in AGA. This has been especially true for determining if reduced blood circulation is a consequence of AGA… or a cause.
As a hair enters the catagen (resting) phase of the hair cycle, the order of operations is as follows: mesodermal tissues surrounding the hair shaft expand, thereby constricting hair shaft growth space. This stops hair growth and signals to the hair’s dermal papilla and microvascular networks to degenerate. So in the catagen phase of the hair cycle, hair growth stops before blood flow reduces… meaning that reduced blood flow is an effect of hair loss… not a cause.
AGA scalps have 2.6 times lower subcutaneous blood flow versus non-balding scalps. And since catagen hairs and early stage AGA hairs look so similar, AGA researchers have used catagen findings as a basis to argue that reduced blood flow is an effect of AGA –not a cause. In other words, these researchers surmise that reduced circulation happens after a hair disappears.
However, there are issues with this line of thinking.
The biggest problem is that in AGA, reductions to blood flow might not only occur in the small blood vessels supporting miniaturizing hair follicles. Rather, they might also occur as a result of the pinching of arterial branches that pass through the scalp perimeter muscles. This occurs due to the involuntary and chronic contraction the scalp perimeter muscles. Therefore, in balding scalps, we have reductions to blood flow in (at least) two places.
In fact, studies on Botox as a therapy for AGA demonstrate that by relaxing these muscles (and thereby improving blood flow through these purportedly pinched arterial branches, and thereby the scalp), AGA outcomes improve… and within the ballpark of what we see with finasteride (although no head-to-head study has been conducted!).
Therefore, reduced blood flow might be a consequence of AGA-related hair follicle miniaturization in certain locations of the scalp, and simultaneously, a cause of hair follicle miniaturization in other sections. It just depends on your vantage point.
This evidence implicates both muscular contractions and chronic scalp tension as potential accelerators of AGA. While the jury is still out on just how contributive these factors are, there’s growing evidence that we should not ignore them.
The bottom-line:
- We can’t apply histological research of the human hair cycle to hair loss disorders like AGA.
- In AGA, reduced blood flow is probably a cause and consequence of pattern hair loss, depending on where you’re looking.
Any questions? You can reach me in the comments any time.

Rob English is a researcher, medical editor, and the founder of perfecthairhealth.com. He acts as a peer reviewer for scholarly journals and has published five peer-reviewed papers on androgenic alopecia. He writes regularly about the science behind hair loss (and hair growth). Feel free to browse his long-form articles and publications throughout this site.
As always, a fascinating and well-written article!
Thanks for reading, Adrian!
Hi Rob! First its great that you’ve posted after quite some time! I find it exciting when you create a new article almost like xmas day!
So to the queries i have:
1) What causes scalp muscles to be in constant contraction in the first place? And is there a link with genetics because how come we dont see this issue with scalp muscles contracting for guys with no genetic link to hair loss?
2) What about the (sometimes) positive success of minoxidil as a blood flow agent, how does that fit within the explanation you have here?
3) You mentioned DHT here acting as an anti-inflammatory or at least is released to deal with inflamation, are you saying DHT in this case is actually positive and that it isnt agrevating the hair follicles but instead trying to heal it?
If that is the case, then how come you see many people gain success when they reduce serum DHT, for a lot of people reducing DHT stops or even regrows their hair.
Hey Danny,
Thanks for the kind words! And great questions.
1. It’s really hard to say, but it’s likely due to a few factors: 1) androgens, 2) genetics, 3) scalp skull structure / suture settlement, and 4) fascia remodeling. All of these factors have feedback loops that influence the degree of 1) tension, and 2) androgen receptor density and coactivator expression — which may result in a higher propensity for certain men with AGA to have these muscles chronically contracted.
2. I’ve long wondered this too. There’s certainly merit to increasing blood flow to the scalp. But as you’ve picked up on, absolute improvements to blood flow mean nothing. What we really want is an increase in blood that is the result of the regeneration of the microvascular networks and dermal papilla. A better way do this is probably by targeting dermal papilla stem cell expression. Wounding is a great way to do this. There are others as well (I’ll probably mention them in the upcoming articles).
In terms of minoxidil — there are several other purported mechanisms by which minoxidil may improve AGA. Outside of improving circulation, minoxidil also has an effect on increasing prostaglandins, specifically from the prostaglandin E family. Many researchers now believe that this might be the major mechanism by which minoxidil improves AGA. So it’s likely that while minoxidil certainly improves blood flow, its main mechanism might not be that. In any case, it does help marginally to improve blood flow. For instance, rosemary oil seems to work directionally as well as minoxidil — at least according to one study — but its effects are mainly just believed to be from vasodilation. So there’s certainly benefit there.
3. DHT is certainly implicated in AGA pathology, but paradoxically, it encourages hair growth everywhere else in our body. One way that we can actually explain this is that when DHT arrives as an anti-inflammatory agent to a tissue, but that tissue is under chronic tension (i.e., the inflammation is tension-mediated), DHT appears to induce a signaling protein called transforming growth factor beta 1 (TGFB-1). DHT + TGFB-1 is what appears to lead to scar tissue development. So this would actually explain why DHT sort of “backfires” in the scalp. DHT wants to help, but under tension, DHT lays down scar tissue.
Along those lines, any systemic reduction in DHT (i.e., finasteride — a type II 5-alpha reductase inhibitor) should, after a certain threshold, diminish tissue DHT levels. So that’s why DHT reducers are helpful.
Best,
Rob
Wow, good job rob. It had long been a theory of mine, after knowing syntethic DHT steroids are used for wound healing: https://www.ncbi.nlm.nih.gov/pubmed/19170590 that DHT lays down scar tissue which would causes fibrosis.
Might I also add that excess estrogen is inflammatory as you know, but DHT antagonizes and keeps estrogen in balance.
What you describe about blood flow is also very similar to my own conclusions.
That’s why Taurine, which reverses fibrosis, has actually been tested to be more effective than finasteride
Thanks
Hi Rob. I bought your e book and started the massages. Did them for about 4 months as prescribed. My main problem is my vertex and was seeing thinning in that area. Although my top and front have always been thick, in the summer I noticed considerable thinning when the sun was shining down or under harsh light I could see my scalp. I hadn’t noticed it before or within the first couple of months of massaging.
I didn’t notice any hairs being lost as I did the massages or any noticeable hair shedding on my clothes over this period.
Could the massages cause a shock to my scalp and cause telogen effluvium? I stopped because I thought I was maybe causing problems. I now have diffuse thinning on top.
I started rogain a few weeks ago in order to get back what I lost.
Any suggestions?
Hey Mick,
I’m sorry to hear that you’ve experienced additional thinning since starting the massages. It’s tough to say what’s going on without a bit more information. In general, the massages should never lead to a visible increase in hair loss — particularly if minimal shedding is observed during the sessions. So I’m wondering if this is due to a) seasonal hair changes related to the hair cycle, b) the natural progression of AGA, or c) massage-induced.
Since we shouldn’t see shock-loss of telogen effluvium associated with the massages, this suggests that maybe there will be benefit if you try to taper / reduce your massage intensity. Or just drop them for the next little while and see what happens. Also — if you’re using Rogaine, I’d recommend also adding in a 1.5mm, 192-count dermaroller once weekly. Evidence suggests that this will improve hair count 4x versus minoxidil alone. That way, we can maximize your chances of getting back on track with the hair.
Best,
Rob
Great article! I’m looking forward to the article on the AGA-scalp tension theory! 🙂
I think there are generally speaking two ways to look at hair loss or any health related issue. There’s the hard science that looks at very detailed aspects of the pathology and then there’s an approach that looks at the bigger picture (what general changes in the environment did happen to get you there etc, not necessarily less scientific).
I think the scalp tension theory and specifically the arguments you laid out in your articles give a very fitting explanation and make sense regarding both approaches.
I recently stumbled upon articles about strength training in relation to flexibility.
For example: https://www.webmd.com/fitness-exercise/news/20100604/resistance-training-improves-flexibility-too
It pretty much says that full range resistance training results in increased flexibility on par with (sometimes even better) stretching. “Full range” seems to be very important in contrast to chronic contraction from for example stress. So one reason why we loose flexibility in this area could be due to a decline in consumption of hard chewable foods. I think that’s really interesting and could be another piece of the chronic tension theory.
I’d be really interested in hearing your thoughts about this. I didn’t really have the time to dig deeper into this yet unfortunately, but hopefully in the future.
Best,
Tim
Thanks Tim!
I think you’re on to something re: jaw development, skull structure, AGA tensile projections, etc. As we age, there’s a constant feedback loop between our skull development and mechanical stress (i.e., mechanotransduction). I hope the upcoming articles better elucidate your question! They should be ready in the next two weeks.
Best,
Rob
So are you saying all we need to do is use botox on our scalp?
I feel its still all about genetics at the end of the day, the genetic model of hair loss fits everything tbh, it explains why homeless men may still have their hair, it explains why fat unhealthy men still have their hair/hairline the list goes on, and there is a ton of evidence supporting it like for example even you have amazing hair, yes you was thinning but you say your dad has his hair, so for you it was probably just some health issue that you corrected with your diet approach (Thyroid etc) and as for the massages it likely just gave a bit more blood flow to the area.
I mean come on, you see professional athletes who are extremely healthy, they dont live sedentary, have the correct nutrition for their biology, in the prime of bodily fitness and im sure they also make their bodies more ‘flexible’ which can lessen the strain from bad posture on the scalp, yet you have some of them go bald and or are balding, i can list soccer players, basketball players and im sure when you look at it their dad probably had hair loss issues, in fact a soccer player called arjen robben is completely bald and hes one of the best players in the world, but guess what his dad is exactly the same, completely bald.
If anything dht probably travels to the scalp in response to the genes being activated by age as it is meant to do so purely from an age standpoint, like how we start getting wrinkles as we age, hair loss probably triggers in response to general aging, its just a bad gene that gets triggered by age. I mean even for myself, my dad had really thick hair at 19 same as me and he lost the majority of his at around 24/25 exactly whats happening with me.
Hey Milik,
Genetics are certainly a big factor (probably the biggest)! Genes + environmental inputs are what determine gene expression, and that’s what determines everything from how tall we are to the tensile projections at the tops of our scalps to our propensity to respond to inflammation with DHT. Because of this, it would make sense for AGA to run in the family, and affect sons at roughly the same age as it affected fathers (since skull structure, suture settlement, etc. are largely genetically determined).
Botox injections certainly aren’t a cure-all for AGA. I wish it were that simple! Botox just goes after one target (i.e., contracted muscles) of several involved in AGA pathology.
Best,
Rob
Hi Rob,
Thank you for producing this research.
I’ve read your articles on contracted scalp muscles and hair-loss.
Are you now at a stage in which you recommend a course of action?
Would it include botox, scalp massage, DHT inhibitors (if tolerated) and derma-rolling?
** Apologies if you’ve already answered this question
Thanks Anonymous. It really comes down to personal preferences — i.e., finances, daily time commitment to a regimen, etc. All of what you’ve mentioned are very viable options, and certainly synergistic. In my interview with Dr. Freund, he mentioned that the lifts he would see from men doing Botox + finasteride, minoxidil, or both were sometimes 50%+ increases to hair count. But again, Botox is expensive — and finasteride always comes accompanied with caveats.
Hey Rob,Great Article,my question for you..
What do you think is the best approach in case of AGA?
Thanks Bob. It’s hard to say! It depends on your comfortability with AGA drugs, time commitments to treatment, and finances. Generally I think mechanostimulation + FDA-approved drugs are a great start, but mechanical exercises on their own also reap results. What is your current hair regimen?
Just wanted to say keep up the good work Rob! Your efforts are appreciated by many!
Thank you Wyatt! I appreciate the comment.
Good to see you back, Rob, though no doubt you’re busy in the background.
So, would it be fair to assume back and sides in respect of massage are arguably most important?
Hey BB — thank you! And yes. There’s certainly a few mechanisms at play with the massages. In thinning regions (the top of the scalp), we have acute wounding / stretching — which promotes growth factor expression (i.e., VEGF-A), dermal papilla stem cell proliferation, etc. Along the scalp perimeter, we have the the relaxation of chronically involuntarily tensed muscles — which improves scalp tension, blood flow, etc. The people who are getting the best results are targeting both.
Huge fan Rob of your work and it is good to see you back, there seems to be quite a few people who are awaiting your response in the other articles I’ve noticed too.
I was personally wondering because i heard it somewhere in one of the comments on another article that you were making a new updated version of the book, is there any possible dates we could have or any updates in general about upcoming things we could get excited about, perhaps that could be an added section on this website like you have the book and article section, perhaps a news section or something to keep us updated on what you’re up to these days, just a thought.
Anyway all the best!
Thanks Derek! Yes, I’m behind on comments and emails, but am making a push to catch up with everyone this week.
I’m still working on a major update to the book, and I don’t yet know when it will be ready. Hopefully within the next two months! Otherwise, I agree with your idea idea to have a section of the site explaining what I’m currently working on. I’ll certainly add that soon (probably as part of an About Me page). Thanks for the advice!
It’s interesting how you were opposed to finnasteride etc in the past but seem to be ok with it now.
Im curious to know hows your journey going? Are the massages still working?
Hey Hasan — all is well over here. Finasteride and minoxidil are certainly viable options for AGA, but it’s all context-specific. I think finasteride is over-prescribed, and oftentimes for types of hair loss that have nothing to do with androgens. You also have to weigh the potential benefits of finasteride with its risks. For instance, it’s recommended that someone not conceive while taking finasteride, and I believe the wash-out period is 1-3 months before it’s okay to start trying. Hair gains from finasteride only last as long as you continue taking it, with an expectation that anything maintained or regrown will be lost within 3-12 months after stopping its use. So, for someone trying to conceive in the near-future, finasteride is probably a bad bet. Moreover, you also have to weigh the potential for long-term side effects (brain fog, sexual dysfunction, gynecomastia, etc.) against any maintained hair. But again, finasteride / minoxidil certainly works well, and it may have synergistic effects with mechanical stimulation.
Everything is fine on this end. I’ve personally been experimenting with little-to-no massage work to see how long results maintain in the absence of any therapy. The massages are still working, and hopefully, we should be publishing our data very soon.
Best,
Rob
Hi Rob,
If DHT accumulates and causes scar tissue progressively, wouldn’t finasteride users not have this scar build up?
Therefore how is it they can keep their hair whilst on the drug but then lose it all in a very short period from ceasing the drug? Surely the scar tissue would not accumulate in this short period of time and stop the hair?
So does means that we should make a change in the protocol proposed in the book? How can we translate that into real life actions? Anyway I am in Holiday in thailand, i came from Europe and I am shedding like 300/400 hairs at day, is there any reason for it??
Hey Alex,
The current book appears to be working for most people, so as long as you’re following the demonstration video, you should be moving in the right direction. I’m also working on a book update which will get into more specifics about improving results. In terms of the shedding — this could be from any number of things, but given the context of travel, it sounds potentially telogen effluvium-related. This could be from any number of things (chronically reduced sleep / sleep quality, weight loss, a parasitic infection, gut dysbiosis, etc.). In other words, anything that chronically increases stress (and thereby cortisol).
Best,
Rob
Great article Rob.
Does this is indicate that nutrition and dietry approaches to AGA, will be minimal in effect ?
We have a cause ,which going by your hypothesis could be caused by post pubertal skull bone growth causing tension , inflammation and tissue remodeling.
A healthy diet will be minimal it seems in reversing MPB. While a mechanical approach would help significantly.
This could explain why even healthy people can’t reverse MPB. And why unhealthy people still have hair.
Thanks
Kind regards
Paz
Hey Paz,
Thank you. I think nutrition / diet certainly have a place in improving overall health and reducing systemic inflammation. But as far as improving AGA with diet / nutrition, I think we’re extremely limited. While the occurrences are less common, we still see bald indigenous men who have gone their entire lives with a diet and lifestyle the western world idolizes. My current stance is that AGA is mediated through both genetics and androgens, and is essentially a structurally-induced (and thereby localized) problem. And that’s not to say that it’s irreversible. We’ve certainly seen cases of full AGA recovery (even by accident) in the medical literature. And just as you said, while a dietary approach is likely to have a minimal effect, maybe a mechanical approach will help significantly.
Best,
Rob
Guys. Please try these stretches:
https://livehealthy.chron.com/stretch-head-muscles-relieve-tightness-4140.html
After reading Rob’s article, I instantly decided to tackle the muscle tightness. Understanding that your neck and trap muscles attach on top of the scull.
Despite my pretty typical presentation of pattern loss, I have slightly more on the right side —- interestingly, the right hand side of my neck was tighter.
I also however have an autoimmune disorder which has fused joints in my spine – reducing mobility and most-probably blood flow for a number of reasons.
However in some ways this just further supports a lot of Rob’s articles. I’m doing everything Rob suggests, and although its not been long enough to see results, my general health has improved.
Thanks Rob.
Excellent article, Rob. My MPB started in my late teens, coincidentally the same time when my facial structure started getting more masculine. Along with hairloss I also experienced intense itching and dandruff. Why is itching and dandruff sometimes associative with MPB? Is it because of the increased sebum triggered by androgens?
Thanks Scott! And it’s hard to say where the MPB “itch” and dandruff fall into play. But there are a few things going on that might explain both.
The first is that androgens increase sebum production, so as we enter into puberty and see a surge in androgens, we’re also going to start producing more oily scalp skin. Sebum is the food of choice for a lot of pathogenic bacteria. In fact, when certain bacteria colonize sebaceous ducts, they regulate their food supply (sebum) by producing toxic byproducts, evoking an inflammatory response (i.e., acne), which signals the body to produce even more sebum — and the cycle continues. The end-result: a lot of itching and dead skin shedding in regions that are most likely to be affected by MPB.
Another possibility is that the dandruff is an inflammatory byproduct of the tension in scalp skin, and the dandruff is exclusively what causes the itching. We don’t yet know with certainty yet!
Best,
Rob
Hi Rob,
I am incredibly enthusiastic with your studies and your commitment to reverse Hair Loss. It has completely changed my perception of hairloss and motivation to do something about it. I have been doing Tom Hagerty´s exercises for 14 months and the massages for 6 weeks now. With TH exercises, I was able to reduce hairloss significantly and even get a little regrowth visible on my temples. With the massages, it is too early to say if it is leading to any progress but I continue to see new terminal hair popping at my temples. I have a few questions that I haven´t been able to find the answer to:
1. If calcification could be partly due to pinching blood vessels, could the massages be promoting calcification?
2. When I went hard with the massages, my scalp dried up (used to be very greasy), is this somewhat related to subcutaneous fat and hence could be bad for hair follicles?
3. In the paper, you mention a that once there is a dettachment of the APM from a hair follicle, hair loss may be permanent. Are there other cases in which a follicle cannot be reactivated?
4. You have mentioned several surveys with results and degree of progress, between people implementing the massages. Would it be possible for you to share the data?
Many thanks
Hey Pedro,
Thanks for the kind words. I apologize — I’m realizing now that I haven’t replied to your previous comments in other articles. I’m a bit behind and am doing my best to catch up now. If you have any other questions, please feel free to ask.
1. Right now, the evidence suggests that acute inflammation generated during a massage session (or microneedling) differs significantly from chronic inflammation in balding scalp tissues. Massage-mediated acute inflammation likely increases growth factors like VEGF-A and encourages stem cell proliferation for the dermal papilla (similar to a PRP session). On the other hand, chronic inflammation (the kind generated from skin tension) likely increases a different set of signaling proteins and hormones — which leads to tissue remodeling (scar tissue). The former likely helps with scar tissue, the latter likely causes it. So as of right now, I’m not worried about the massages evoking more fibrosis or calcification.
2. This is commonly reported! It seems like after a few weeks/months of massaging, the sebaceous glands downregulate sebum production — which is probably why you noticed a less greasy scalp. I think it unrelated to subcutaneous fat.
3. Full AGA recoveries have been documented in the medical literature — one of them happening by accident after a 78-year old bald man fell off a rocking chair, hit his head on hot coals, burned his scalp, and in the healing process, regrew his entire juvenile hairline. As a result, I think AGA recovery is possible at any Norwood stage — and regardless of whether the APM has detached. It’s just a matter of uncovering the right mechanisms!
4. Yes! The data is currently in peer review. If the paper is accepted for publication, I’ll opt to publish it as “open access” so that everyone can benefit from the information.
Best,
Rob
Hi Rob,
Sometimes I feel related of what has been documented for anorexia. I just see myself as bald (eventhough I might be NW3 or 4) and ashamed of not having a full head of hair. I do not know why, but it affects my confidence, perhaps my self esteem as well. What I want to tell you is thank you for your response and help. I will continue with the massages (almost 3 months into them) and just started dermarrolling as well.
No doubt I will let you know about my progress and continue being part of this great community that has built around your investigation and experience.
Best, and please let me know if you have information about the timeframe for the paper with the data (the one that is currently in peer review) and also about your next article.
Thanks Pedro! RE: the paper — I should have some answers for you VERY soon! Best of luck with everything and please keep us all posted.
All my best,
Rob
Hey Rob,
I found an article dating back to 1997 from lifextension magazine and it mentions an explanation of an old model? Of MPB that i thought might be interesting to share and im not sure if its still relevant but here is the passage:
‘The latest scientific model to explain baldness involves the action of dihydrotestosterone (DHT)-the major metabolite of the male hormone testosterone. Scientists have found that excessive secretion of DHT stimulates a localized immune reaction, which, in turn, generates an inflammatory response that damages hair follicles, resulting in their miniaturization and eventual loss.
What appears to happen is that DHT (and, perhaps, other androgenic hormones) causes the immune system to react to the hair follicles in the affected areas as foreign bodies. This is suggested by the presence of hair follicle antibodies as well as by the infiltration of immune system cells around the hair follicles of balding men and women.
Blood vessel diseases such as atherosclerosis may also contribute to accelerated hair loss, as evidenced by the higher incidence of these diseases in balding persons.
Successful prevention and treatment of accelerated hair loss necessitates dealing with some, if not all, of these factors involved in the process, except for the genetic component of baldness.
The use of anti-androgens by themselves generally produces a very limited degree of hair regrowth. However, they are necessary and useful as adjuvants to other therapies such as hair-growth stimulators and oxygen free radical scavengers.
The immune response provoked by male hormones such as DHT probably plays the most significant role in balding. Stimulated by androgens, the immune system targets hair follicles in genetically susceptible areas to cause the premature loss of hair characteristic of male pattern baldness and other forms of accelerated hair loss.
Thus, a side effect of the immunosuppressive drug cyclosporine (which is used to prevent the rejection of transplanted organs) is scalp hair regrowth. It may be that cyclosporine is the most potent single hair regrowth agent known. But the drug causes potentially severe toxic side effects when used systemically, including kidney damage, hypertension (high blood pressure)-and even death-which precludes its use as a hair growth stimulant. However, other ways (with no potential for system toxicity) have been found to inhibit the localized immune response that leads to hair loss.
There are many pharmaceutical agents (such as Rogaine) which can stimulate a degree of hair regrowth in some people. However, none of them alone can produce the kind of cosmetic benefits that balding people desire. What’s needed is a multi-modal approach to hair treatment that combines anti-androgens with autoimmune protective agents, oxygen free radical inhibitors, and other hair growth stimulators to halt hair loss and generate hair regrowth to a degree well beyond the abilities of single compounds.’
This was targeted towards selling Dr Peter Proctors research and work but was wondering if the whole immune response could be an angle we haven’t looked too much at.
I stumbled upon this when i found out that some people who had male pattern baldness actually regrew their hair back from using immunosuppresant drugs and so i thought how can that be the case if its mainly DHT and the other scalp tension issues, calcification/fibrosis etc, i haven’t see this being mentioned much but thought it interesting to share.
All the best!
Thanks James! I appreciate the comment. I know a researcher at Oxford who’s studying exactly what you’re describing. His hope is to find a target without the severe side effects of cyclosporine — maybe something localized to just the scalp skin. I’ll try to get him for an interview on the site.
Wow yeh that would be amazing!
Yeh i think its something to do with the wnt1 pathway which connects to hair growth, something called the sonic hedghog protein, i think its this pathway that scientists are looking to target, looks interesting.
Rob,
I am also a huge fan of your work. I have been following your blog for a while but it wasn’t until about 2 months ago that I began tackling hair loss seriously. I have been slowly losing hair since i was in my late twenties. I am now 37 and not ready to shave it all off yet. It was pointed out by my barber that I had lost even more hair in the span of a month (which I am sure was do to a life changing traumatic event).
I would guess I am about a NW4. For 7 weeks, have been derma rolling with a 1.5mm roller. I had been massaging (pinching, kneading, pressing) just the crown and forehead areas as best I can (usually with a towel) as those areas are tight. Gradually, the sore spot at the top of my head went away and I think the hair fall has stopped. I do have dandruff and shampoo once a week with nizoral. I rinse daily with cold water.
Maybe it was the timing, but this artical really spoke to me about the muscles at the periphery of the skull being contracted and tightening the skin, just like a drum. (Don’t know how I missed that in the hormone therapy piece).
I had been neglecting to massage those muscles and only massaging the balding areas. So, 2 nights ago, I went to town on my whole head. After, I did not notice any soreness in the frontalis muscles, very light soreness in the occipital region. But when it came to the periauricular region and the temporalis muscles, holy moly was it sore. I may have over done it as I had a lump on the left side of my head which disappeared in 2 days.
I am wondering if the periauricular region reacted that way because they were chronically tense? And contributing to the “drum head” effect? I have suffered from migraines and tension headaches my whole life.
Anyway, keep up the stellar work! Hair loss sucks. Your work (along with some others) has given me the motivation and sparked a glimmer of hope that I can do something. I know it takes time to regrow and I am hoping I will see something here in the next couples of months. Definitely requires a lot of patience especially coming from where I am.
Hey Rob,
congratulations on another great article – I’ll read it in depth as soon as I find the time. I’d love to see an article on microneedling. I’ve seen lots of really impressive results on hair loss forums lately.
Kind regards
Manuel
Hi Rob – I really appreciate your work on this topic and I’m sure it is changing many lives for the better since this is genuine research based analysis and it is not one of those pharma-backed rip-offs that all hair loss sufferers have gotten used to.
I haven’t actually purchased your book but based on reading most of your articles, I started out with what I think is your protocol and I must say that the results are becoming positively obvious. I’m approaching 4 months doing the massages and almost 2+ months with the weekly dermaroller. I have had two family members say that I have noticeable hair growth and I agree! I will keep the massages going for another few months before reducing the duration since it is fairly difficult and tiring to do 40 mins each day.
Can you please write up an article on dermarolling as you have eluded to in a few of your comment responses? I want to get your take on that in-depth. Keep up the good work and a big thank you!
Hi Rob
Can you please elaborate why AGA comes from an inflammation. How you define inflammation?
Thanks
Dirk
Hey Rob,
Just wanted to share this looks very interesting and is relevant with your article here:
https://www.hairlosstalk.com/interact/threads/involvement-of-mechanical-stress-in-androgenetic-alopecia-von-mises-2d-analysis-models.113276/?fbclid=IwAR0kGSnH3Mpq0uQjfJuNDJ_9L5MVzAN9rgPJBa8E6up97eBEf_XrjSnnYoc
Hi Rob,
Please write a detailed article on derma-rolling and derma-stamping? Everything from preparation of the scalp to use/no use of topicals, to what technique, needle length to use, etc.
Thanks
As usual, excellent article. You’re a legend man!
Hi rob
I started using Rosemary oil with massage process , and I use it only for the corners of my head every night before bedtime,do you think it’s enough i use rosemary once a day? And i use it without any carrier oil
Hello Rob,
Here you are again with an great article.
I have tried the scalp massages for two months and my scalp felt allot looser after that time. Its so time consuming that i couldnt keep it up so i stopped.
I than started taking saw palmetto. Pumpkin seed oil and grape seed extract. My scalp tension never came back and im glad it didnt because it seems my hair finally is starting to grow stronger again.
“DHT is certainly implicated in AGA pathology, but paradoxically, it encourages hair growth everywhere else in our body. ”
Great article Rob, but with this line, I don’t feel it’s so much of a paradox.
Scalp hair and body hair are different in the sense that scalp hair is terminal from early ages (in the absence of significant DHT), while the body hair remains vellus, only selectively becoming terminal in puberty and later life in response to DHT, with its pattern and follicular sensitivity to androgens determined by gender and genetics.
So, it stands to reason body hair that is present as a secondary sex characteristic responds to growth from increasing levels of DHT, whereas scalp hair is terminal in children and therefore grows without requiring a response to DHT. This should make us question whether scalp hair in later life really responds in the same way to DHT as body hair does, given DHT’s primary purpose is to trigger androgenic changes, not general indiscriminate hair growth. It is not like the presence of DHT turns all vellus body hairs terminal, only where androgen sensitivity is genetically expressed.
It seems obvious that scalp hair, not being androgenic in nature, does not require DHT to grow healthy and thick as in juveniles, and may not respond the same way as body hair follices do to DHT. I agree with your hair loss model 100%, and none of this is in contradiction to it, but I would not be surprised if it turns out DHT had no growth promoting effects on scalp hair follices, or even had a negative effect as most believe. I don’t have a reference on hand, but I do remember some study proving the link between scalp hair miniaturization and DHT, though this may of been ex vivo and away from the other scalp environment factors. Simply put, when you consider scalp hair and androgenic hair as different, with different triggering requirements, the discrepancy in the action of DHT is no longer a paradox.
this man used an electric massager and got results. thoughts ?
https://vitamindwiki.com/Vitamin+D+reduces+hair+loss
Hi, thanks for the article! Question: in your opinion – in androgenic allopecia does fibrosis happen mostly in hair follicles, or also in the scalp tissue outside hair follicles?
Thanks, Ben
Hey Rob, love your work and sincerely appreciate everything youre doing. I’ve come to a second wave of motivation to solve my hairloss problem as the first attempt was not a sincere full attempt. Im going to be obviously incorporating your stuff and a bit of ray peats. Will keep you informed on progress.
2 things, did you say you were going to start a forum where we could discuss your ideas? if so did you want me to help you with a secret facebook group, its quick and easy and once its done you simply can email all of your customers the link we can start our community.
and lastly, would love your thoughts on this forum post. Man apparently has hit the magical protocol for decalcification and has had some impressive results, his ideas mostly align with yours, have a read when you get the time. “https://www.evolutionary.org/forums/anabolic-steroids-peds/hair-loss-dht-steroids-think-again-very-interesting-topic-28623-2.html.”
Hello Rob, with your massages I managed to repopulate something in the crown area, but I still have many entries. I wanted to ask you about the micropigmentation technique … have you seen any case in person? It seems realistic?
Yes of course! I know it is a tattoo, but i have never seen it in person. Does it look real?
micropigmentation is a tattoo my dude
Hi Rob, great article as always 🙂
I feel that you are right in that scalp tension causes bad things for our hair.
Hormones are most certainly at work here as well as scalp tension.
Whether that’s in more extreme skull growth/remodelling or something else.
Those eunuchs and others who were injected with T certainly underwent major changes from hormones as they stated losing hair.
Most guys won’t lose hair until after puberty.
Post menopause women and post mid life men seem most at risk of hair loss and this seems to be a hormone related issue more than anything.
Also the fibrosis idea seems right too but it isn’t isolated to our scalps alone as heart/artery problems go hand in hand with hair loss in men.
The last post before me made by Kevin had a link to an article which has interesting ideas about calcification and is a good read.
This fibrosis/calcification is something we experience all over our body it seems.
In saying all this, you would have forgotten more than I will ever know and your work is invaluable 🙂
Rob what do you think of this product made by hairlossrevolution
Do you think it could replace the manual massages sessions and just do this twice a day for 20 mins each session?
Looks like this sort of device would definately help with the chronic scalp tension, I just wonder if 10 minutes per day would help enough to make a difference? I wouldn’t mind an easier way than massages. I’ll probably order one after Xmas.
yes, I would think that 20 min x 2 a day would be better.
Thanks so much for the share bro! I believe calcification cannot be forgotten.
I Mean even mpb is linked to increased risk for heart disease its all over news sites when you google, but of course it wont be the hair loss itself that increases the risk but must be the ‘calcification’ and in this case to the arteries and the affects to the heart long-term makes so much sense!
Hi Rob, been doing your exercises since march 2018 along with most of your dietary advice. I’ve basically regrown most of the hair that I lost. Is there anywhere I can send/post the before and after photos?
It would be great to see some more positive results, definitely need a forum to share progress pics . Glad you’re doing well, I’m 5 months in but not growing any new hairs yet. Seeing some pics would certainly inspire me to kick on
I agree a forum would be great!
Hi anyone with knowledge about this regime with dermarolling. I’m wanting to add dermarolling once a fortnight, but not sure how long to stop and restart massages before and after if I do so? I’m struggling with massages in the crown area, it’s not loosening up in that area after 5 months. Wondering f I could derma that one area, lost a lot of hair after Minix and need a plan to get something going again in that one spot. Cheers
Would I be able to send those photos to me too ? Would love to see the progress
Hi Rob
Please start a private forum for all your clients who’ve bought your packages so we can trouble shoot and support each other. Seeing each others progress photos would really motivate and help us.
Have you tried cupping on the scalp to induce stress, increase blood flow and to break up calcification?
Could it help or work?
Hi rob definitely think a forum is needed!
Hi John Lee. Are you replying to me? Hard to tell who’s replying to who in some of these comments. Cheers if so. Also agree with everyone else who thinks we need a forum, we definitely need support. It’s also good for Rob if we succeed and can show it
Hi Rob,
Just letting everyone know that I have purchased the growband and will update readers on my use of the product. Looking forward to the forum as well.
@Alan congrats on your purchase mate. I wish you success and please keep us posted.
Thanks Rob
Just read a lot of your articles. Very helpful and offers a different perspective than the current options I was aware of (Finasteride, Rogain Saw Palmetto). In the absence of knowing which direction to go I have tried to take a few different approaches.
Currently taking propecia, saw palmetto, and a Nizorall dadruf shampoo. I am going to look at massage therapy and dermarolling.
I am also going to try rosemary oil and punpkin seed oil. for those, is it topical application with massage hat works best and how many days a week would you reccommed.
I am trying to find DHT inhibitors, a DHT blocker, and also improving blood flow with scalp therapy. Is there a set of approaches that you would recommend to help simplify the approach?
I just found your site this week so will do a bit more research and pick up a copy of your book.
Thank you
Hi Rob, you have a ton of messages here haha.
Hey, I would recommend you DO NOT start a forum.
Oh man, forums are how great things die.
It will mean you get to have less and less contact with people directly because of high numbers.
You will have little control who is doing what because of high numbers.
Then there is the “community” that will spring up out of it.
Those who believe that because they have been around the longest, that they have positions of forum authority.
Often they become forum moderators, and become self proclaimed experts or never make it to moderator and just post as though they are experts anyway
Just look at what happens at the other hair loss sites.
So very sad and so very avoidable.
pretty negatively skewed perception of a forum. lets talk about some positives, people share progress, people share personal protocols and how they managed to fix their own problems, which may/may not spark a lightbulb moment for the reader, seeing other people succeed will in turn boost your motivation to as well, people are able to quote Rob on a more easily accessible platform, so Rob’s information disperses at a faster rate to a wider audience. More traffic = huge growth for the community and results drives attraction which will ultimately be beneficial for everyone. we need a forum, period.
Hey Kevin — I agree, but I can totally see where Andrew is coming from. It’s important that we don’t let our community become what most other hair loss forums have become. I think I’ve found a good way of setting this up, and will have more to share with everyone soon. Thank you for the great ideas.
Andrew, I disagree with your comment. The problem is Rob does not have the time to speak to every single person individually, we need to bounce his ideas off people that are having good results. I’m 5 months in and losing a lot of my hair, without other people’s help I am struggling to go on. Rob is one guy who had pretty good hair to begin with, I want to talk to guys who’ve come back from far worse situations and get their advice too. We’re talking about people who read Rob’s book and are using his approach, not a forum about every other idea on the internet. And as you said in your message, look how many unanswered messages there are. Some of us need more help, so I think it’s a great idea personally. And there may be tons of before and after pictures out there, at this stage I’ve seen about 4 people’s pictures on the main page. Get your point, but it can work
Hi, I found this research, how can you explain this study?
“The author transplanted composite skin grafts from balding, non-balding, and bald areas of the scalp, to the skin of the arm. The galea aponeurotica was trimmed away from the grafts. The patient was a 29-yr-old male with progresive male pattern baldness (male pattern baldness). The transplants from the balding area became bald at the same rate as the balding donor site in the receding frontal, hairline, whereas the transplants taken from the non-balding area in the occiput continued to grow the same amount and quality of terminal hairs. Bald grafts taken in front of the receding hairline remained bald. This shows that the cause of male pattern baldness lies in the follicle itself or in its very close surrounding and does not depend on the galea aponeurotica, the increased tension of the scalp or of its muscles, the diminished vascular supply to the scalp or any other regional factor localized to the head area. It also shows that the ‘balding clock’ keeps time even when the follicle is transplanted to another region of the body.”
in Acta Dermato Venereologica 59(3):266-8 · February 1979
Richard I concur with you. I’m a female with diffuse AGA. I spent a lot of time surfing other hairloss forums and to my surprise found a few comments and success stories of Robs clients personally posted by them there. Why? Maybe partly because they don’t have an outlet to discuss their successes and techniques here. All of them had positive things to say so I can’t see why having a forum here would be a bad thing. We as Rob’s customers need an outlet here to unite and help and support each other. Alot of failed hairloss forums have one thing in common – just hair loss which translates into insults and mud slinging between members. But Robs customers have both hair loss and a firm belief in his research and protocol. I’m sure all the concerns that Andrew has can be dealt with. Like closed FB groups each member would obviously be an existing customer but can also fill out a quick questionnaire for admin to see if they can be admitted as members. This would gather all the genuine members who have a positive attitude and same the values in one place and avoid too much conflict. And if the forum becomes a war zone then yes Rob can decide to delete it.
Hi Anna. Yeah, totally agree with you. It would be easy to go to any number of hair loss forums and start up a discussion about this approach, but you open yourself up to every other practitioner bringing in their ideas and disrupting the conversation. I want to try this approach 100%, but I don’t know if I’m doing it right from day to day. Just need help with the finer details, and you want answers immediately if you run into problems. I’m all for experimenting, but why not use the guys who are 3-4 years into this approach for advice. I will certainly give it if I’m successful. At this stage I’m following the 2 success stories from the book, unfortunately I didn’t even read them until a few weeks ago. So I had to make changes 4 months in that would have been great from the get go. I definitely believe in this, just need to battle past this 5 month point where the minoxidil is now totally out of my system and has taken all that hair with it. Hoping for some improvement in the next 2 months. Cheers Anna
Like Ale above, I would also like to hear thoughts on why hairs transplanted from scalp to arm continue to behave as they would (whether terminal or shrinking) if they had remained in the scalp.
With this being the case I can see how maintenance through scalp massage would be possible if the massage somehow prevented the follicle’s epigenetic switch into miniaturisation from being triggered, but regrowth must not be possible from massage alone if a miniaturizing hair is unable to benefit even if it is moved to ideal conditions (I’ve never known people’s arms to bald).
Then again, it also begs the question how Propecia/Minoxidil regrows hair for some people (Can we be certain of this even? Says the skeptic).
If I could reconcile this with Rob’s method, I might be inclined to go all in and purchase the book.
I would also dearly like an explanation for this. It is the one piece of research that prevents me from going all in and commiting to purchasing Rob’s protocol.
A forum is not going to make Rob respond any faster with the time he has.
Spamming this message list with requests for a forum or other unimportant comments and chatter only makes this problem worse. Keep your messages focused and on topic.
A little respect for Rob, please.
Hi everyone,
Firstly, I wanted to apologize for being way behind on answering emails and comments. I’m not yet in a position to respond to everyone, but I promise I’ve read all of your commentary and will get back to you as soon as I have time.
There are a few reasons for my delays.
The first reason is that I’m finishing another article to answer people’s questions about hair transplantation studies and how their findings seemingly contradict the scalp tension hypothesis. Once that’s published, I’m hoping I can answer all of those questions in one swoop.
The second reason is that I’m in the middle of addressing peer reviewers’ comments for our second manuscript, which I hope to publish within the next couple of months. This is based on the survey data we collected on readers last year.
The third reason is that I’m in the middle of another major book rewrite, which includes a new book, new videos, more success stories, 20+ reader case studies, interview transcripts with other AGA researchers, and a forum. The new information will be based on our first (and hopefully, second) paper — and the insights from the latest crop of best responders.
Finally, I’ve also been trying to redesign the website to make it look nicer and load faster. A reader recently told me that while she loves the site’s content, the design and feel makes it appear as though it was thrown together by a middle schooler. I agree with her. I’m not a website designer and have prioritized researching / writing over site aesthetics. Now it’s time to make things look nicer.
All of this — on top of my regular job — has set me back a couple of months in terms of emails and comment support. I apologize again. I hate that I’ve left everyone hanging. In any case, here is the big comment I wanted to address–
To Anna, Richard, Hasan, Michael, and any others advocating for a forum–
I agree. If set up correctly, a forum will do so much for our community. I want everyone to have access to our success stories — to ask them questions, learn from their mistakes, and maximize their chances for regrowth. Right now, there’s no way for us to interact aside from article comments. This is probably why we have so many off-topic questions in each article — which I’m sure gets annoying to the people here. We need a gateway to interact, give off-topic questions a home, and provide a roadmap for new readers to find answers to previously asked questions.
A forum is the perfect tool to facilitate these interactions. But it has to be set up correctly.
Andrew — your points are heard and well-taken. Forums can turn extremely negative. A forum has to be set up in a way that stops it from becoming Reddit’s tressless. I have some ideas on how to do this, but I’m also open to hearing others’ opinions. When the forum is launched, I promise there will be measures in place to stop it from turning counterproductive. Richard has offered some great insights. Another mandate might be that the forum is only open to those who’ve read the book… so that we can keep advancing the knowledge within our community, rather than repeating much of what we already know.
I’ll have more updates to come within the next two months. In the meantime, please look for an article in the next week!
Best,
Rob
Thanks for the update Rob, excellent news! I’m all for a private forum for people who have purchased the book and are using your methods, the tricky part as you say is actually setting it up. Would be great for potential customers to see a community forum attached to the site, or as part of the purchase . I must have logged into Gumroad a hundred times to read the book and watch the videos, don’t suppose it could be attached to that page somehow? Anyway, looking forward to the new and ever evolving info in the future, for now I’m quite happy I’ve finally found a routine I like after 5 months of trials with the massage. Reading Jarrods success story a month ago was huge, I was definitely overdoing it and making it worse . And half hearted with the diet to compound it. Feel good now, have high hopes moving forward. At this stage I’m thinking why did I use minoxidil for 30 years, although I’ve lost some hair in the 4- 5 months since, I see some tiny potential this week. Ok, thanks again Rob, and good luck moving forward. Maybe an assistant? Cheers
Hi Rob,
I bought your book a couple of years ago (it’s about 105 pages with a 5 min demonstration video) – I see the new book is 250+ pages with a 15 min video. have you added any new advice (other than FAQs and feedback from current users) – or has there been any updates to the method etc.?ALSO, you mention your email address is in the book – but it doesn’t feature in the one I have (it’ll be great if you could drop me an email).
Thanks,
Kunal
Mumbai, India
Hello.
I know this is off topic, but bone broth contains collagen, and isn’t excess collagen something we don’t want? I drink my broth daily, but thought about it today.
Hey Andreas! The benefits of consuming collagen are derived, in part, from improving glycine:methionine ratios. The excessive collagen we see in AGA is in the form of disorganized cross-hatchings (i.e., scar tissue / fibrosis). It’s the result of an inflammatory process — which doesn’t share overlap with collagen consumption. So drink all the bone broth you’d like!
Hi Andreas. Interesting point, maybe it depends on the daily amount? I think a cup a day is great for gut health and inflammation, no idea if it’s enough to affect your hair. I thought collagen was a good thing for hair strength, hope so as I drink it everyday
Howdy Rob, RE forum, a monthly or yearly subscription fee and/or purchase of your book to qualify.
Keep the price high so you are not only rewarded for your time but it will keep only serious members on board.
Most time wasters won’t foot the bill.
Danny Roddy charged $25 per month for direct success, I think something like that would be good as an access fee.
I’m poor but I think keeping the members to those willing to pay will keep quality high.
🙂
I disagree with charging high fees. If that’s the case I might as well book a Skype consult with Rob. Charging a fee could help him maintain the forum but it would need to be reasonable to be accessible to a greater spectrum of members. A high price would make it unattainable to alot of poor and middle class folk who are following Rob’s programme and whom he also aims to help. Also don’t forget Robs foreign customers who are hampered by exchange rates. I certainly cannot afford $25/month in forum fees based on the country where I currently reside. I’ve also heard a lot of people complain about certain famous hair loss specialists who’s fees are so pricey their services they’re being deemed exploitive and are almost only available to the wealthy. Remember the aim of the forum that some of us are proposing is to help each other as Robs customers reach our goals, to convince, to motivate and encourage- not make the forum more exclusive.
Also please remember someone entering the forum may only be a temporary visitor and have one or two questions with something that’s hampering his/her progress and then leave. Would they really be expected to pay fees just for that?
Hey Rob, I find your article and the physiology/pathology you lay out to be very fascinating and compelling. I also like that you entertain critiques of your theory which not a lot of people are willing to do.
What is your take on obstructive sleep apnea’s potential effect on hair? I had a thick head of hair at 19-20. For various reasons, I overate and gained over 100 pounds over the last 5 years and find myself thinning and receding profusely whereas the rest of my family all still seem to have their hair. I was recently diagnosed with severe sleep apnea. Could this contribute to AGA?
Kamran,
Your sleep apnea is probably a symptom of the general state of your health, rather than a cause for sleep apnea.
Losing the weight progressively, getting a nutrient rich diet, making sure you’re not deficient in vitamin D, and doing the massage as described by Rob in the book is likely to solve your problems within a year or so. If you give it a shot that is.
Hi Rob,
We are desperate! My 16 year old son has lost lots of hair after worrying himself silly for a year about having a brain tumor, when eventually after tests and many arguments with docs, it was inflammation of the nasal sinuses! We are dermabrasing, using supplements, dht blocking shampoos, he is doing headstands/ inversion table twice daily, massage etc. the fallout has slowed but I think he may have a copper overload as he tries to eat healthy and supplements and nuts contain copper? He eats pumpkin seeds and takes a quercertin and lycopene supplement as this is supposed to quell the DHT. We are using salicylic acid to get rid of the grease on his scalp.
1. Calcification – apparently natto (fermented soya) stops natural calcification, can you look into this? Also do you need to cut out dairy/calcium foods to stop the build up? I give my son milk, cheese for protein as this is what is needed for hair growth isn’t it? 2. You mention nicotinomide, helps form alpha reductase, should he then stop consuming this in foods etc? 3. You mention botox can you please give details of the areas the botox needs to be injected into the scalp? 4. Rosemary and peppermint is it best to consume it or apply via essential oils (I put couple of drops of rosemary in our shampoos) 5. Gonna take him off the supplements and use nettle and green tea again. Many thanks
hey look into getting a hair mineral analysis test from TEI, hair best indicator for seeing our balance of minerals and whether we are a fast oxidizer or slow oxidizer. Fast oxider means we have a fast oxidation rate and so fast metablosim and slow oxidizer is slow metabolism. I got mine done and funny enough I was high in calcium compared to magnesium as well my zinc was slow. I been on the diet and plan now and feeling the shedding slowing down, only been on it for 2 months but other people on a private fourm i trialing and getting improve din their hair and thyroid . Try it out your son is young and will be able to fix it quick
Hi Rob
Couple of other questions – 1. Can you dermabrase too much? my son does 1.25mm every 3 days, would you suggest longer intervals or a 1.5mm less often? 2. He uses apple cider vinegar as a rinse )and I try to get him to drink a tspn of it in water) Any hints on getting rid of grease as massage stimulates the grease glands and must make it harder for the little hairs to grow through? 3. He’s been taking ashwaghanda last 4 months which has been his saviour as he says it has stopped him worrying. definately stopping the hair supplement.
Many thanks
Lorraine Cartledge
Hey Ale,
Thanks for reaching out. It’s a great question, and the answer isn’t so straight-forward. As such, I’ve just finished writing two articles to help explain things:
https://perfecthairhealth.com/scalp-tension-hair-loss/
https://perfecthairhealth.com/hair-transplants-debunk-scalp-tension-hair-loss/
Best,
Rob
Hi Lorraine , doing too much could also hinder results. Especially with what I assume is dermarolling, and massages. How often are these done ? The scalp needs healing time aswell.
Could his hair loss be temporary TE due to stress and worry , in which case he could see recovery within a year or so.
16 is a very young age. Tackling calcification straight away might not be the right course due to his age.
What type of hair loss is he experiencing.
Is is it thinning all over or standard pattern loss.
A greasy scalp is the first thing to tackle.
1. Wash hair with cold water
2. Do massage
3. Eat more anti inflammatory foods.
4. Stick with dht natural blockers and ashwaghanda.
Your approach seems far to aggressive , which could hinder healing.
Just my two scents. But Rob should answer in much better detail .
Good luck
Hey Rob!
I bought your book awhile back and im having to have another go at the massages. I struggled with consistency and when i was constant it seemed to backfire (i must of been overwhelming my scalp).
In regards to this article, when it says the perimeter of the scalp, can this be interpreted as the ridges? and so would the massage that targets the back and sides with the additional 3 min ridge pinches be more beneficial than originally perceived?
Also one more question, we spoke via email and you said a new book was coming out. Just wondering if that’s still in the works because I would like to upgrade my package once it comes out.
Thanks always.
Hi Rob,
Today marks exactly 12 weeks since I purchased Perfect Hair Health and began your method of scalp massages. I have been consistent, missing only 2 sessions in that time (due to a nasty gastro bug!). I am absolutely BLOWN away by the results so far. I don’t know if my results are typical, but my hair fall began to decrease after several weeks, and within 4 weeks, it had decreased to less than half of what it had been for, essentially going back to what was “normal”. The regrowth is significant, especially on the side-part/temporal regions. I am seeing regrowth of hair that has been absent for over 2 years. I am especially seeing a lot of 1-2 cm long hair, and there is already a noticeable increase in the diameter of that new hair at the scalp compared to the tip. In this area, where I had typically had more gray, it seems to be growing in darker as well.
Having spent countless hours on internet research, I was initially impressed when I first found your website and saw the volume of research you had done, and felt sure you were correct in your theories. I am now even more convinced. I look forward to the next few months, and to our video chat (which I have not scheduled yet). I hope to give you even more information that you can use to help others who have been struggling with this very real, very mortifying, very perplexing, very devastating issue of hair loss. Thank you, Rob.
Hi Lisa, I’m a fellow female sufferer of AGA. I’ve been using Rob’s techniques since November 2018. I’m not sure about my own results as I have very sneaky and slow diffuse thinning but no bald batches yet so can’t say if I have any regrowth. I’m really happy for you though as I read that Rob’s techniques can take a bit longer to show on females than males. I’ve also fell off the wagon for a few days due to the rush of the December Holidays but slowly re-introducing the massages back in my routine. I noticed a few things though. My hair which was quite oily at the beginning of the massages has become quite dry within a matter of weeks. I’ve been using Nizoral shampoo for months but my shampooing has now lately decreased from 3 to 2 times a week since the massages. My shedding during the massage also decreased from quite a bit to an average of 10 strands per session which is not too bad. So think it could be showing signs of changing my scalp’s environment. Being female, is there anything that you think triggered your AGA? The derm told me mine is purely genetic but I can trace it back from when I changed from the anti-androgen oral contraceptive Pill being Diane 35 to a Pill containing a mild androgen called Gestodene.
Hi Anna. So sorry–I’m just now seeing your reply to my post. You asked if I had an idea of the cause of my hair loss. I’ll try to be brief. I’m a 52 y.o. female with healthful lifestyle habits. I am a personal fitness trainer and have been fit essentially all my life. I exercise with cardio and/or weight training 6 to 7 days a week, and have maintained my body weight/fitness levels all my life. I have never smoked or drank. Zero drugs except the occasional ibuprofen or antibiotics. I tried birth control in my late twenties, and it did not work for me.
When I noticed minor hair thinning (and graying!) on my side part about 2 yrs ago, and what seemed to be a slight loss in overall volume, I suspected perimenopause. Because of other symptoms(low energy, painful intercourse), my internist put me on the lowest dose of femhrt in 2/2018. Starting in July, my hair loss went out of control and persisted until shortly after I started Rob’s program in October. Up until October, I did research tirelessly, trying to establish a connection between the hormonal therapy and hair loss because I had no explanation for it. Hair loss is not prevalent in my family. I had multiple blood tests including thyroid and ferritin levels. Suffice it to say I came away frustrated. Nothing was conclusive. When I found Rob’s research , I was relieved because I had vindication for my frustration over the multiple contradictions I had found in the theories of hair loss. (Side note: I was also taking every vitamin supplement that anyone was recommending for hair loss! Nothing was working.) I hit a low point in October 2018 when my derm said my scalp biopsy revealed AGA, and prescribed Spironolactone which I would have to take for the rest of my life. I got a copy of the lab report and found that she had not told me the truth. The dx of AGA was not even conclusive. She had essentially lied to me, and took the easy way out by prescribing a medication that would lower my already extremely low blood pressure. The side effects were completely unacceptable, and hair regrowth was not even guaranteed since it was being prescribed off-label! I decided that I would rather be bald than take this drug.
Thankfully, I found Rob’s website. When I read Rob’s book, light bulbs started coming on. Because of my experience with muscle cell stimulation via massage and exercise, I knew that Rob was on to something. An honest evaluation of my lifestyle revealed that my scalp had been receiving virtually no manual stimulation to speak of. For the last 5 years, I was only washing my hair every 4 days, whereas previously I had been washing it every other if not every day.(Once I noticed the hair loss, I was even more gentle with shampooing and brushing so as to not lose more hair. As if!) I checked my scalp, and it was indeed very very tight. I could not even pinch it. I found a few other lifestyle changes I need to make, including getting more sleep and reincorporating inversion time.
I am now at week 23 of the massages and other lifestyle changes, and as I posted on another article of Rob’s, my regrowth is what I would consider unbelievable–my hair stylist was shocked–and my scalp is so much more pliable. Since I began the massages, I have performed about 80-90% of them inverted. I think this has made a difference. I have only missed a handful of massages in that time. I’m looking forward to seeing Rob’s hard data on the other participants in his program, because I feel that his findings can completely revolutionize what is believed about hair loss, and approaches to regrowth.
I am very conservative and cannot tolerate hype–in all of my years as a trainer, I have never sold a single supplement. (Another impressive thing about Rob–he does not promise overnight results. He clearly says it will take months to see anything. It takes time yo change yhe hair follicle.) My clients and friends and family know me as someone who verifies before endorsing, therefore, I will continue a few more months before I start recommending it to my friends dealing with hair loss. I believe that my success is due in part to my starting this therapy so early on in my hair loss. I want everyone to know about his research.
Congratulations Lisa! This is great news. I followed up with you via email. I look forward to our Skype call, and I’m so happy to hear that things are working well for you. Please keep us updated!
Best,
Rob
Hi Rob – does supplements like whey protein, creatine in any affect hair growth (or exacerbate hair fall). I have heard some concerns around creatine, but apparently there isn’t any conclusive research (especially at about 5 gm/day). Do you have any views around either? If so, are there any alternatives which are safe from a hair perspective and continue to give benefits in muscle building.
Thanks!
Hey K,
Creatine raises serum DHT, but its effects on DHT conversion in the peripheries (i.e., scalp tissues) are still unstudied. So it’s hard to say.
Unfortunately, marketers lead us to believe that whey protein and creatine are necessary supplements for muscle-building and workout recovery. I can promise you that this isn’t the case.
The right diet, sleep, stress reduction, sprints, sunlight, and bodyweight workouts are really all we need to see significant muscular gains. I’d avoid these supplements entirely — not because of their potential effects on hair, but because they’re unnecessary and expensive.
Best,
Rob
Hi Rob,
I bought your book a couple of years ago (it’s about 105 pages with a 5 min demonstration video) – I see the new book is 250+ pages with a 15 min video. have you added any new advice (other than FAQs and feedback from current users) – or has there been any updates to the method etc.?
It’s mostly the FAQ and more details. Same method.
Thanks Lorrie. I’ve been hesitant to comment on the band — mainly because nearly all other readers have reported the opposite of you: that the GrowBand is hard to use, doesn’t compress / grip well against the scalp, that the manual labor involved is annoying, and that the makers severely underestimate / downplay the time requirements to actually see results.
For instance, the manufacturers benchmark users with a goal of 10 minutes daily, but the GrowBand is an exact replica / knock-off of the Takeda Medex device — which only showed regrowth in one study after 3-12 months of use at 2+ hours daily.
For what it’s worth, I think the idea behind a tension-relief band is great. But given the above, I can’t stand behind that particular product — at least from what other readers here have mentioned so far.
Thanks for sharing your perspective!
Best,
Rob
what do you think about hair cell apoptosis by Activation of caspase 3 which is triggered by dht and tgf, decreased proliferation of keratinocytes and do you think there’s anything changed in the genes of hair follicle cell as it miniaturizes after transplanted to another part of the body?
Not trying to be funny here but could cialis or vigra help with hair loss if used over time?
It works by increasing blood flow so there may be something in it.
Hi Lorrie! Unfortunately, that website (hairlossrevolution.com) is riddled with typos, half-truths, plagiarism and ludicrous anecdotes, which makes me think twice about buying anything from them. Did you really notice an improvement in scalp laxity after 2.5 months of usage? And isn’t the product ridiculously overpriced at $297?
Thanks Lorrie. Does it ‘cover’ all parts of the scalp? My concern is that it might not be as targeted as fingers. Glad to hear that it’s working for you.
Hello ! I have a question for you if you don’t mind :
I don’t know English very well and I struggle understanding the conclusion about the “scar tissues” that would cause the hair to fall.
I bought a microneedling device, would this help reducing these scar tissues ? Or may it worsen the situation ?
Thank you !
Hey Maxime,
The overwhelming amount of research (at least right now) suggests that micro-wounding can actually improve scar tissue! I know that’s paradoxical, as scars are a consequence of an inflammatory stimulus. But our propensity to scar is actually determined by wound size and the growth factors, hormones, and signaling proteins upregulated during the repair process. With small acute wounds over old scars, we can actually leverage a set of substances that help to improve / partially diminish that pre-existing scar tissue during the repair process. However, if the wounds are too large, a different set of substances are upregulated and, resultantly, we might see scarring. So, it’s all about finding the right wound-healing balance.
It’s this set of principles that partially explain why massaging, microneedling, and platelet-rich plasma therapy (PRP) can help improve our hair.
Thank you very much for your reply !
Hi Rob,
There is a guy from hair loss is reversible website his name is Tom haggerty. Tom haggerty maintained his hair throughout his entire life by the alternating contraction of the frontalis and occipitalis muscles. Isn’t this article contradicting Tom haggerty’s scalp exercise.
I hope you understand what I mean, and sorry for the language English isn’t my native language.
Hey Kainan,
I believe Tom Hagerty’s exercises can improve AGA outcomes, but not for the reasons he ascribes on his website.
Tom Hagerty suggests that his alternation exercises (done for 5-20 minutes per day) help strengthen the scalp perimeter muscles and, during their engagement, improve blood flow to the scalp… thereby improving hair loss. These exercises have anecdotally helped a lot of people, but my issues with this mechanistic explanation are that the effects of improved blood flow are likely too short-lived to have any measurable impact on our hair.
Take minoxidil, for example. One of its suspected mechanisms is improved blood flow. Minoxidil’s half-life is 22 hours, and it’s recommended to be applied twice-daily so that its effect is constantly happening. Now compare this to the Tom Hagerty exercises: 5-20 minutes of improved blood flow… maybe some lingering effects 10-20 minutes after the exercise. It just doesn’t seem to add up that this mechanism alone would explain its helpfulness for our hair.
Now think of something else the Tom Hagerty exercises do. Over a series of months, they teach us to become aware of our scalp perimeter muscles, and specifically, how to relax them when we’re not doing the exercises. Almost anyone who’s tried the Tom Hagerty exercises for a series of months reports that their scalp feels more relaxed during their time away from the exercises, and that they have better control over these muscle groups. In this case, the anecdotes of the exercises make sense – because the relaxation of these muscles sustains improved blood flow for much longer than the actual exercise intervals.
Long-story short: it’s likely not that the TH exercises engage these muscles and thereby improve blood flow to the scalp and thereby improve our hair loss. Rather, it’s likely that the TH exercises teach us how to control these muscles and intuitively relax them outside of the exercises… leading to more sustained blood flow improvements and thereby better hair.
Best,
Rob
This explains everything except those who take steroids and never lose their hair.
I would assume serum dht levels would leech into the follicles and skin and cause fibrosis all over the body? Or am I wrong?
Would getting botox in my forehead only help?
Hey Tarek,
It seems like the effects of DHT, at least in regard to the development of fibrosis, are highly dependent on the expression of androgen receptors and the degree of DHT that binds to those androgen receptors. This process may also involve androgen receptor co-factors (like the Hic-55 co-factor), and unfortunately, we don’t yet have enough research to extrapolate the mouse models studying these interactions to men with AGA. In short: while these differences might explain why men with higher “DHT sensitivity” seem to see higher rates of prostate enlargement, atherosclerosis, and pattern hair loss… we don’t yet have great evidence to answer your question yet beyond the “genetic predisposition + environment” blanket answer.
Botox into the forehead might help, but to achieve full scalp relaxation, you really need to target all scalp perimeter muscles. This usually requires 100-150 units of Botox, and unfortunately, it gets expensive!
Best,
Rob
Hi Rob,
I am trying a multi pronged approach to help fix the hair loss since a few days, and I believe it is working, but will wait for some more time to give you confirmed results. I would like to have your inputs on them.
1) I am using dry cupping(aka chinese cupping/hijamah) which involves applying oil to the hair and using a small plastic/glass cup with a vacuum (I use a small hand operated vacuum device) daily to the balding/thinning patches. This is to improve blood circulation, and also relax the scalp muscles with a massage like effect due to the vacuum pull. I think this gives me better results than massaging, probably due to the ‘pull’ force on blood that is much more compared to the normal blood pressure pull available due to a massage or a head stand :/.
2) Adding supplements to my diet like Biotin, B vitamins, Iron, collagen, calcium + VitD3 , and enough protein to ensure that the right nutrients are available.
3) Adopting an Intermittent fasting eating plan to help reduce inflammation.
Please can you advise me on the above approach, and/or if you see any concerns with it.
Thanks,
Armaan
You are on to something with this analysis and it definitely relates to my hair shedding imo. I’m 39, both my parents have tons of hair so genetics can’t be the catalyst to my hair problems. I recently went through a stressful time that caused extreme tension around my head (felt like my head was capped), possibly due to a virus. I developed brain fog, head pressure etc. I’ve lost 60% of my hair in 7 months. My scalp still doesn’t feel the same.
Hi Rob,
Very interesting article. With your flow diagram model outlined above, I can see it all starts with the genetic factors / DHT leading to an increase in scalp tension. This would explain why only people with chronically tight scalps can lose hair in a way related to AGA right? I’ve often thought why wouldn’t other people lose their hair through this mechanism, as how can my scalp be more tight than anyone else’s. And also there must be a relationship (as you have researched on) between the factor of epigenetics as I have started to lose my hair in a similar pattern my dad is, but this only started in his 40s, and I am 28 (gradually over the last few years).
In my head, the factor which holds most true, is that I’m sure DHT may bind to people’s follicles who do not show any hair fall, and so ultimately only those genetically sensitive see hair fall related to DHT.. what are your thoughts here?
Thanks for reading, Tom.