A complete guide to diffuse hair loss
Diffuse thinning isn’t a type of hair loss. Rather, it’s a term used to describe the appearance of someone’s hair loss.
When someone has diffuse hair loss, it means that they’re experiencing a decrease in hair density across the entire scalp. Many people first notice diffuse thinning as a wider part, a thinner ponytail, or after seeing more scalp skin following a haircut.
In this article, we’ll uncover what diffuse thinning is, what causes it, and what can we can do about it.
For what it’s worth, I’m intimately familiar with this presentation of hair loss. It was part of my hair loss diagnosis back in 2007. At the time, my dermatologist diagnosed me with male pattern hair loss, also known as androgenic alopecia (AGA). He also attributed my diffuse thinning exclusively to AGA.
What I didn’t learn (until years later) is that diffuse thinning isn’t just linked to AGA; it’s also associated with dozens of underlying chronic conditions – hypothyroidism, heavy metal toxicities, nutrient deficiencies, and more – each of which has a unique set of causes, and a unique set of treatments.
Consequently, diffuse thinners are at a high risk of getting diagnosed with the wrong type of hair loss… because their hair loss presentation overlaps with so many different causes.
If I’d known this – and if I’d known how to troubleshoot which underlying drivers of diffuse hair loss were relevant to me – I could’ve saved myself a lot of time, money, and hair.
That’s why I’ve written this article – to help you avoid my mistakes. By the end, you’ll learn:
- The major causes of diffuse thinning (and the ones commonly missed by doctors)
- Ways to identify which causes might be relevant to your diffuse thinning
- Why it’s critical to test first, treat second (Ben M.’s story)
- How there may be an “order of operations” for reversing diffuse hair loss, at least if we suspect multiple causes
The good news? If we can properly identify and address the underlying causes of diffuse thinning, we can often see full hair loss reversals. We’ve got case reports from the scientific literature – and the case studies from readers – to prove it.
What is diffuse thinning?
Diffuse thinning is a term used to describe a decrease to hair density across the entire scalp. This can happen as a result of:
- Each individual hair strand getting thinner (i.e., hair follicle miniaturization). As each hair grows thinner, this creates the appearance of general thinning everywhere.
- An increase in hair shedding (i.e., a decrease in the total number of hairs on the scalp). If we’re constantly shedding more hair than we’re replacing, then over time, we lose hair density.
In either case, diffuse hair loss leads to thinner-looking hair, with more scalp showing (particularly when the hair is parted).
Diffuse thinning in a female scalp

What causes diffuse hair loss?
The causes of diffuse thinning are widespread. Here are some of the most common culprits:
- Genetics & hormonal imbalances. Diffuse hair loss can occur from due to polycystic ovarian syndrome or menopause in women, and/or pattern hair loss in both men and women.
- Stress. This includes mental, emotional, and physiological stress – childbirth, illness, surgery, chronic anxiety, and even physical exhaustion.
- Chronic conditions. Diffuse thinning is often observed alongside conditions like hypothyroidism, hyperparathyroidism, gut dysbiosis, nutrient deficiencies & surpluses, and heavy metal toxicities (more on these later).
How do I identify my unique causes of diffuse thinning?
The short-answer: it’s complicated.
There are many types of hair loss, and each type has a different set of causes, and a different set of treatments. If we apply the wrong set of treatments to the wrong set of causes, we won’t see much regrowth.
So, how can we go about identifying the causes of diffuse hair loss? In reality, there are two approaches.
Approach #1: visit a qualified dermatologist
The first approach is to find a qualified dermatologist who (1) specializes in hair loss disorders, and (2) conducts full health evaluations. This health examination may include self-assessment questionnaires and a range of lab tests. This would allow for a highly trained individual to vet the appearance of our hair loss against our health history – and tell us which causes of diffuse thinning might be most pertinent to us.
Unfortunately, it’s difficult to find a dermatologist who does this.
For starters, not all dermatologists are involved in the “academic” side of their field. As such, many are years behind the literature on how to best diagnose and/or treat certain hair disorders.
Secondly, dermatologists have to run a business. This means they can’t spend an hour with every patient. So, they ask patients the minimum number of questions to get them 80% of the information they need to ascertain a diagnosis. This works well for maximizing patient visits and revenue; it doesn’t always work well for the patient with a complicated case of hair loss.
Lastly, insurance companies are frugal; they limit the lab tests you can order for patients. So, even if a dermatologist wanted to get more specific in their diagnosis by ordering lab work, health insurance may not let them do so.
All of this is to the detriment of the person sitting in their chair – their patient.
I would know; I’ve personally experienced all of this during my visit with a dermatologist to investigate my diffuse thinning, and my subsequent hair loss diagnosis.
When a dermatologist falls short of the right hair loss diagnosis (my story)
In 2007, I noticed a significant amount of hair loss. I experienced very slight temple recession, but significant hair loss at the crown and to my overall hair density. So, I visited a leading dermatologist in Massachusetts to understand what was going on.
Within 15 seconds of combing through my scalp, that dermatologist diagnosed me with androgenic alopecia (AGA) – specifically, AGA in a diffuse pattern as well as crown thinning.
This dermatologist did not ask me about any underlying health questions. I wasn’t asked if I was taking any drugs or supplements; I wasn’t asked if my family had a history of chronic conditions associated with hair loss; I wasn’t given lab work to rule out the possibilities of a thyroid disorder, a vitamin D deficiency, or a heavy metal toxicity from drinking well-water my whole life. (These questions would’ve ruled out other common causes of diffuse thinning.)
Rather, I was handed a diagnosis based exclusively on the presentation of my hair loss: AGA (which happens to be the most common hair loss diagnosis in adult men). If you’re curious, you can see my diagnosis here.
Years later, after investing in thousands of dollars in lab tests, I discovered that my hair loss probably wasn’t exclusively due to AGA. Rather, I likely had AGA alongside chronic telogen effluvium (i.e., diffuse thinning) – the latter of which was linked to subclinical hypothyroidism.
No wonder why interventions for AGA – minoxidil, low-level laser therapy, and saw palmetto – didn’t work for me. I was only treating partly treating the underlying causes of my thinning hair… because I’d only received a partial diagnosis.
Can’t find a good dermatologist? There’s another way!
For those who don’t have access to a top-level dermatologist, there are still ways to help yourself identify why your hair loss is occurring in a diffuse pattern.
It all starts with education.
Specifically, we can employ a DIY-approach to (1) learn about the major causes of diffuse thinning, and then (2) see which causes apply to us as individuals.
Approach #2: learn the major causes of diffuse thinning, and then compare those causes to your own health history and hair loss situation
The rest of this article is designed to help you identify the potential drivers of your diffuse hair loss. It begins with education, and it ends with an action plan to (hopefully) help your hair.
It all starts by diving deeper than diffuse thinning’s appearance – so that we can understand its causes.
Diffuse hair loss: two categories
To reiterate, diffuse hair loss is a term to describe general thinning across the entire top of the scalp. This sort of thinning generally falls into two categories:
- Hair thinning caused by androgenic alopecia (AGA)
- Hair thinning caused by hair shedding disorders
Differentiating between these two types of hair loss is important. After all, each type of hair loss is associated with a different set of causes, and thereby a different set of treatments.
Androgenic alopecia (AGA)
Androgenic alopecia (AGA), also called pattern hair loss, is one of the most commonly diagnosed types of hair loss in the U.S. In fact, some resources estimate that AGA is responsible for up to 95% of hair loss diagnoses in adult men. This is what I was diagnosed with back in 2007.
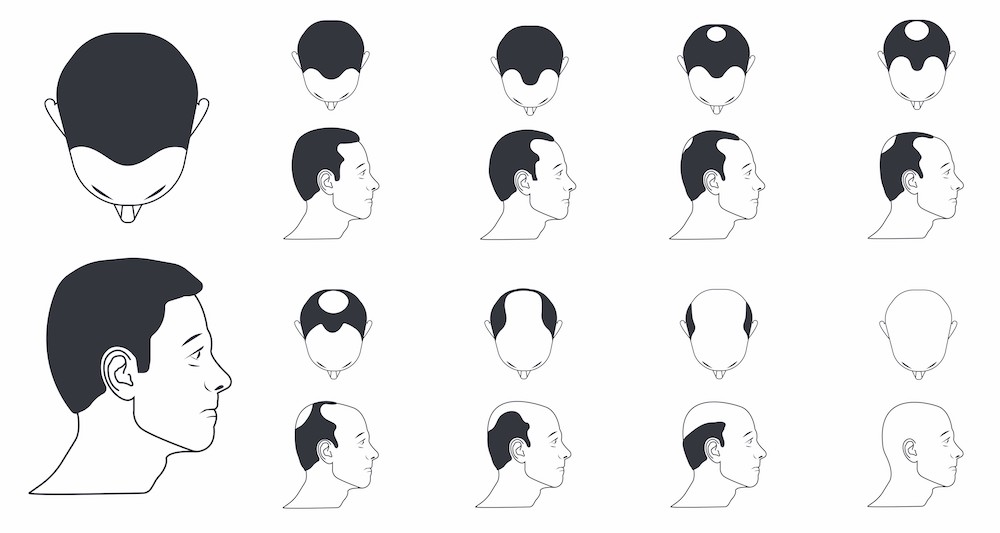
Male pattern hair loss
In men, AGA usually starts from the hair line and/or the crown. This is the reason why terms like “receding hairline” and “bald spots” are common for men with hair loss. This can occur as early as the teen years or early 20s.
Androgenic Alopecia (AGA) Norwood Scale: how AGA progresses in men
But not all AGA cases follow this exact pattern. According to our survey data, 20-40% of men with early-stage pattern hair loss also notice diffuse thinning. So, it’s not uncommon to notice general decreases to hair density that coincide with AGA.
Female pattern hair loss
In contrast to men, the overwhelming majority of women with AGA (female pattern hair loss) don’t notice hairline recession or a bald spot. Rather, they notice an even thinning of hair throughout the top part of the scalp.
Ludwig scale: how AGA progresses in women

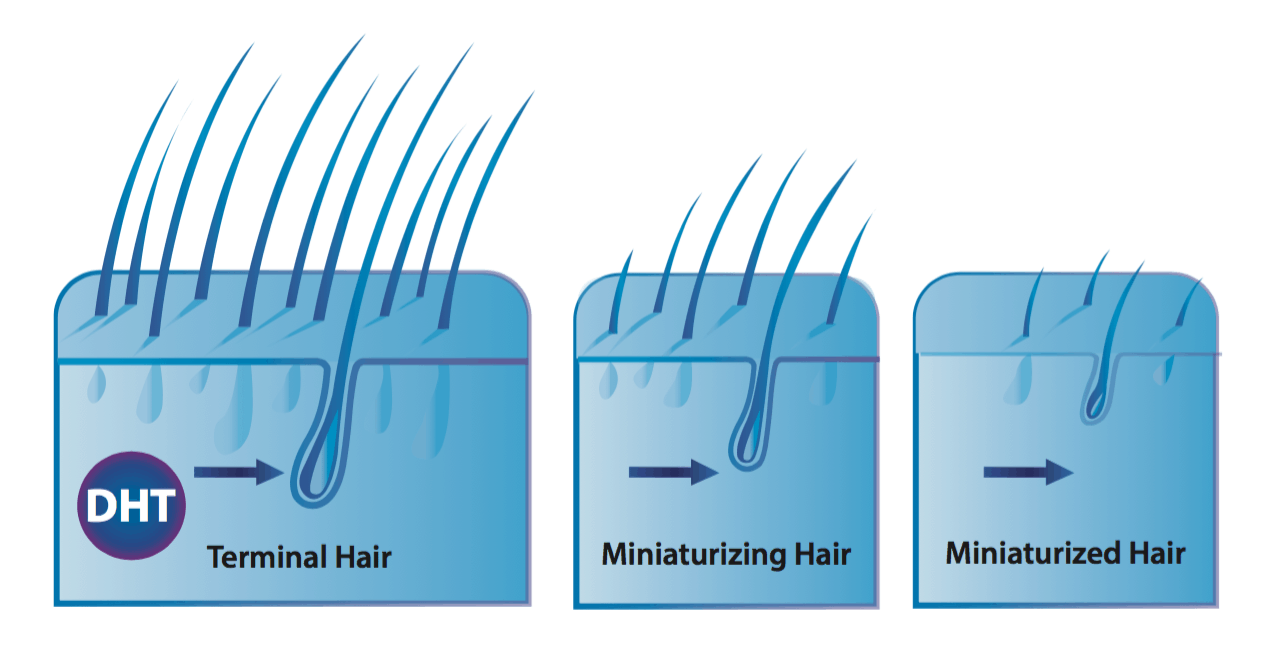
The defining characteristic of pattern hair loss: hair follicle miniaturization
Hair follicle miniaturization is when an individual hair strand, over a series of years, gets thinner and thinner. Researchers mainly attribute this phenomenon to a hormone called dihydrotestosterone, or DHT. When DHT comes into contact with scalp hair follicles that are genetically prone hair follicle miniaturization, these hairs begin to shed, and with each hair cycle, come back thinner and thinner.
Hair follicle miniaturization: each hair strand gets thinner
This is important! Why? Because if you’re noticing that when you shed hair, certain hair strands look thinner and wispier than others, then it likely means that you’re dealing with hair follicle miniaturization. By association, this also means that you’re likely dealing with (at least) some degree of androgenic alopecia.
One thing to note about androgenic alopecia: without treatment, this type of hair loss is chronic and progressive. That means that unless you do something about it, it generally will only get worse.
Summary: one way someone can experience diffuse thinning is through hair follicle miniaturization. This is when each hair strand slowly gets thinner over time. Hair follicle miniaturization is almost always caused by androgenic alopecia: a hormonally- and genetically-driven hair loss disorder. Without treatment, hair follicle miniaturization typically only worsens.
Interestingly, hair follicle miniaturization from androgenic alopecia is just one way diffuse thinning can take place. One other way is through a hair shedding disorder. With hair shedding disorders, you’re not losing hair density due to miniaturization; you’re losing hair density due to excessive hair shedding.
Hair shedding disorders
Hair shedding disorders are when there is an imbalance in the hair cycle; specifically, when too many hairs are shedding, and too few hairs are growing in to replace them.
Throughout the course of a day, it’s normal to shed 100-150+ hairs – even in the absence of a hair loss problem. This is because 10-15% of our hair follicles are constantly in a state of shedding, and after shedding, these hair follicles are then replaced by newer, healthier hairs that will grow in.
Under normal circumstances, our scalps maintain a “homeostasis” between the number of shedding versus growing hairs. This way, we never really notice any changes to hair density – as any hairs shed are quickly replaced.
However, hair shedding disorders occur when this balance becomes out-of-whack. Specifically, when too many hairs start shedding and/or too few hairs start growing in to replace them. Under these circumstances, we see a decrease to overall hair density – and due to hair shedding (rather than hair follicle miniaturization).
On that note, there are two main types of hair shedding disorders: telogen effluvium and chronic telogen effluvium.
Telogen effluvium
Telogen effluvium can occur in men and women, but its the most common type of hair shedding disorder in adult women.
Unlike AGA, telogen effluvium is not due to hair miniaturization; it’s due to a disruption in our hair cycle, which leads to an increase in hair shedding, and thereby a decrease to overall hair density. This can occur quickly or slowly, and it can be temporary or chronic.
In any of these scenarios, diffuse thinning might be the way that telogen effluvium presents.
Acute telogen effluvium
Acute telogen effluvium is a kind of telogen effluvium that is temporary, and generally lasts for less than six months. When its triggers are identified and removed, the hair begins to grow back again and its as if the hair shedding never took place.
So, what are these potential triggers? There are several:
- Mental/physical stress. Studies using animals have shown that physical or mental stress can exert inflammation on hair follicles and massive increases to hair shedding. In humans, this stress is often the loss of a loved one (mental/emotional), or giving birth to a child (physical) – both of which can lead to temporary but dramatic increases to hair shedding.
- Crash diets/weight loss. Hair requires both micronutrients and macronutrients to grow. Severe caloric deficits (as in, crash dieting or prolonged calorie restriction for weight loss) can make it difficult to get enough micronutrients and macronutrients to support hair growth – which can trigger hair shedding. In other words, the hair follicles shut down to conserve nutrients for other places in the body that are more necessary for survival than growing hair.
- Medications. The following medications may interfere with the hair follicle’s natural cycling, and have been linked to acute telogen effluvium:
- Antithyroid drugs
- Tricyclic antidepressants such as amitriptyline
- Bromocriptine
- Levodopa
- Cimetidine
- Amphetamines
- Non-steroidal anti-inflammatory drugs (NSAIDs)
- Hormonal contraceptives / hormone replacement therapies
- Anticoagulant medications (rare)
- Beta-blockers (metoprolol and atenolol)
- ACE inhibitors
Now, these are common triggers of temporary hair shedding that lasts for less than six months. So, what about for hair shedding that has lasted longer for six months?
Well, this isn’t always indicative of acute telogen effluvium. Sometimes it can be the beginning of something known as chronic telogen effluvium (or a combination of both). More on this below.
Chronic telogen effluvium
If you find yourself struggling with diffuse shedding for more than six months, and you don’t see signs of hair follicle miniaturization, then you could be suffering from chronic telogen effluvium.
This is the same premise as acute telogen effluvium: the hair follicle changes its normal hair cycling due to some sort of trigger. However, in these cases, the shedding persists for much longer.
If you haven’t experienced diffuse shedding for 6+ months, it doesn’t necessarily mean you have acute telogen effluvium and not chronic telogen effluvium. It’s just the 6-month mark is when most clinicians start to differentiate between the two.
The causes of chronic telogen effluvium are widespread, and oftentimes tied to underlying chronic conditions. We’ll discuss these below (you may also notice some overlap with the causes of acute telogen effluvium, too).
Hypothyroidism
The thyroid is a gland in the next that plays a role in many, many, many different functions of the body. When the thyroid function begins to slow, meaning it produces less thyroid hormone, one of the consequences can be chronic telogen effluvium.
This study found that thyroid hormone (the production of which is impaired in hypothyroidism) interacts with the hair follicle to participate in stem cell function. Thus, it has a direct impact on the follicle’s ability to produce a hair shaft.
It comes as no surprise, then, that many hypothyroidism patients report suffering from varying degrees of hair loss.
Hyperparathyroidism
The parathyroid, which is located near the thyroid, is responsible for secreting a hormone called parathyroid hormone. Its main role is to regulate calcium levels in the body, however, it also acts as a negative regulator of the hair cycle.
This means that, when the parathyroid hormone binds to parathyroid receptors in the hair follicle, hair growth is inhibited. Suffice it to say, too much parathyroid hormone (in a condition called hyperparathyroidism) can precipitate chronic telogen effluvium.
So, if you find yourself suffering from a hair shedding disorder, hyperparathyroidism could be a possible cause.
Nutrient deficiencies / surpluses / imbalances
Nutrient deficiencies, surpluses, and imbalances are something that can trigger bouts of hair shedding – particularly when prolonged and severe.
There are a variety of causes of nutrient imbalances, and in general, they all boil down to an imbalance between changed demand for nutrients versus changed supply of nutrients.
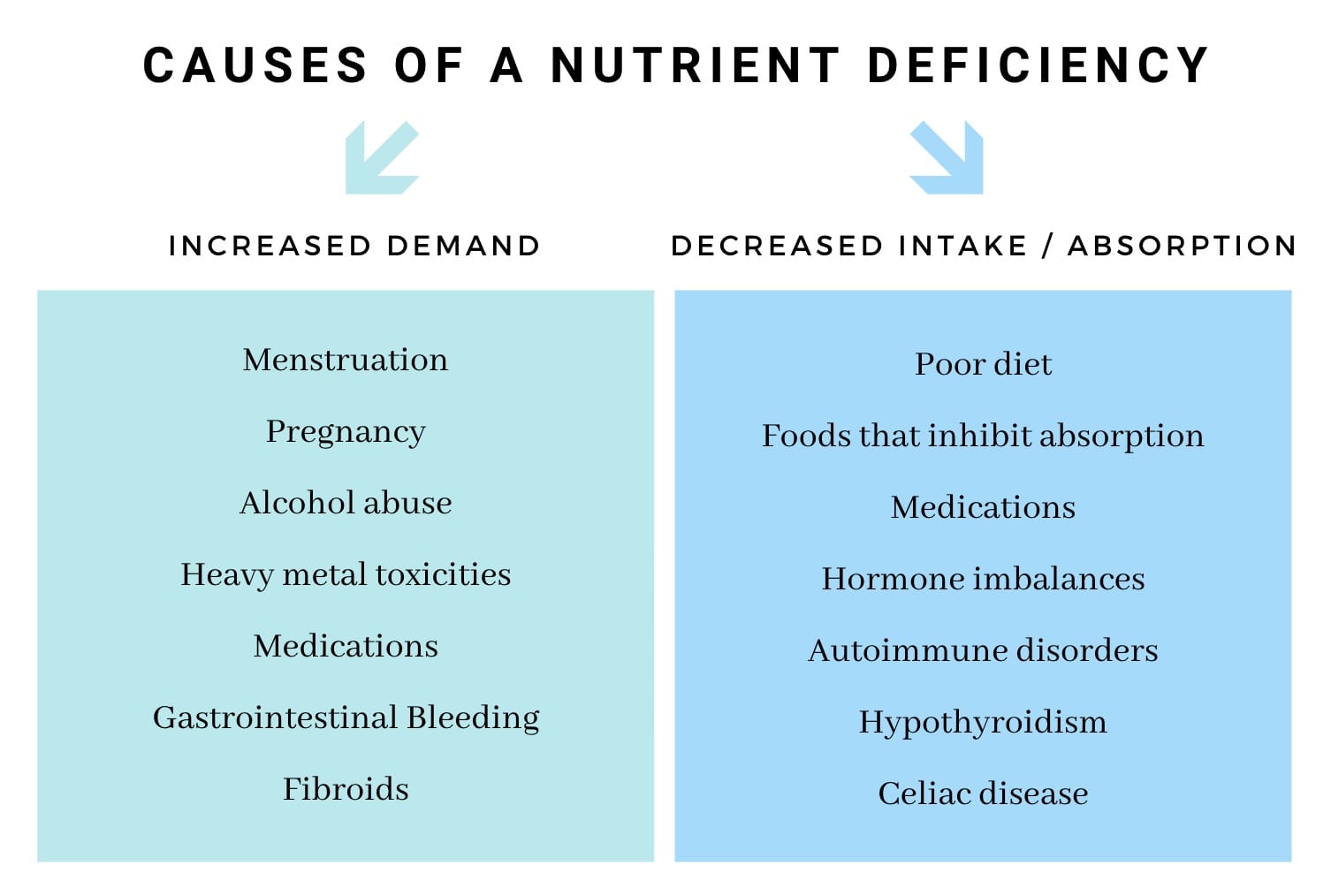
Interestingly, there’s a difference between nutrient imbalances that cause acute telogen effluvium versus nutrient imbalances that cause chronic telogen effluvium.
In acute telogen effluvium, these nutrient imbalances are often the result of poor dietary choices. In chronic telogen effluvium, these nutrient imblances are often the result of underlying conditions: malabsorption, copper IUDs, chronic illnesses which increase the demand for nutrients, etc.
In either scenario, you can end up with hair loss. So it’s important to understand (and rule out) whether a nutrient deficiency is relevant to your specific hair loss case (we’ll reveal steps on how to do this later).
Small intestinal bacterial overgrowth (SIBO)
Small intestinal bacterial overgrowth (SIBO) is a condition whereby the pathogenic bacteria begin overgrow in the small intestine.
This creates issues with nutrient absorption – as these bacteria begin to compete with the nutrients that otherwise would’ve been absorbed by the small intestine and transported elsewhere in the body. Moreover, SIBO also triggers intestinal inflammation – the consequences of which we’re only beginning to understand.
There are currently no studies that tease out the connection between SIBO and hair loss. However, in my experience working with females who have diffuse hair loss, an overwhelming percentage of them who test for SIBO come back with a positive result. So, given the mechanistic links between SIBO and nutrient deficiencies, it’s worth mentioning this chronic condition as a potential trigger to chronic telogen effluvium.
Heavy metal toxicities
Heavy metals – like lead, cadmium, thallium, mercury, arsenic, aluminum, and copper – are often toxic at varying levels of exposure. And unfortunately, many of these heavy metals are linked to hair loss.
The mechanisms by which these metals trigger hair loss differ from one to another. For instance, mercury and thallium bind to proteins that build the hair shafts thus disrupting the proliferation of the hair follicle. Mercury also has a specific affinity for the thyroid. When absorbed into the body, it can downregulate the production of thyroid hormones, leading to hypothyroidism.
Another mechanism by which heavy metals may disrupt hair cycling is through the displacement of essential minerals – like magnesium, calcium, zinc, and iron. Heavy metals can knock essential minerals out of their binding sites – interfering with transport to tissues as well as disrupting the roles these minerals play in cellular activity. This is why heavy metal toxicities can mimic a nutrient deficiency – even in the presence of adequate nutrient consumption and absorption – because the problem is not necessarily in getting the nutrients where they’re supposed to be; it’s keeping them there.
While severe heavy metal toxicity is uncommon in developed countries, we are consistently exposed to heavy metals through our water supply, food, and air as a result of modern manufacturing practices. So, for people who present the symptoms of a heavy metal toxicity, and who have an elevated environmental risk of exposure, it’s usually a good idea to do further testing.
Which brings us to our next step: moving beyond education, and toward action.
What can we do about diffuse hair loss?
Now that we’ve learned of the major common causes of diffuse hair loss, we can go about identifying which ones are relevant to us. There are two ways to do this.
First, we can order laboratory work to test for all of the above “causes” linked to diffuse thinning. This would rule out which causes are relevant to us. Unfortunately, this method of testing is cost-prohibitive. It would cost tens of thousands of dollars to order each and every lab test to give us the insights we need to determine which ones are relevant to our unique hair loss case, and which ones aren’t.
If that doesn’t sound like a worth investment to you, don’t worry. There is another way.
The best approach (aside from working with a doctor)? Compare your environment, health history, and hair loss case against the major causes of diffuse thinning
Now that we’ve handled the educational component of this article, this may be easier than you think.
Simply ask yourself the following questions:
- Is my diffuse hair loss from hair follicle miniaturization, hair shedding, or both? The answers to these questions will help you determine if your diffuse thinning is related to androgenic alopecia, telogen effluvium, or both. And that, in turn, will tell you whether the causes are related to androgens, genetics, temporary stressors, or chronic conditions.
- Do I have any health symptoms in addition to hair loss? And do these symptoms overlap with any chronic conditions linked to hair shedding disorders? This might include things like poor digestion, skin problems, brain fog, cold hands/feet, and beyond.
On that note, we’ve compiled a list of the conditions linked to diffuse hair loss, their symptoms, and how this hair loss might look in the scalp (its speed of onset and presentation). Using this list, it’s likely that you can narrow down your lists of relevant lab tests to just a few orders (if any).
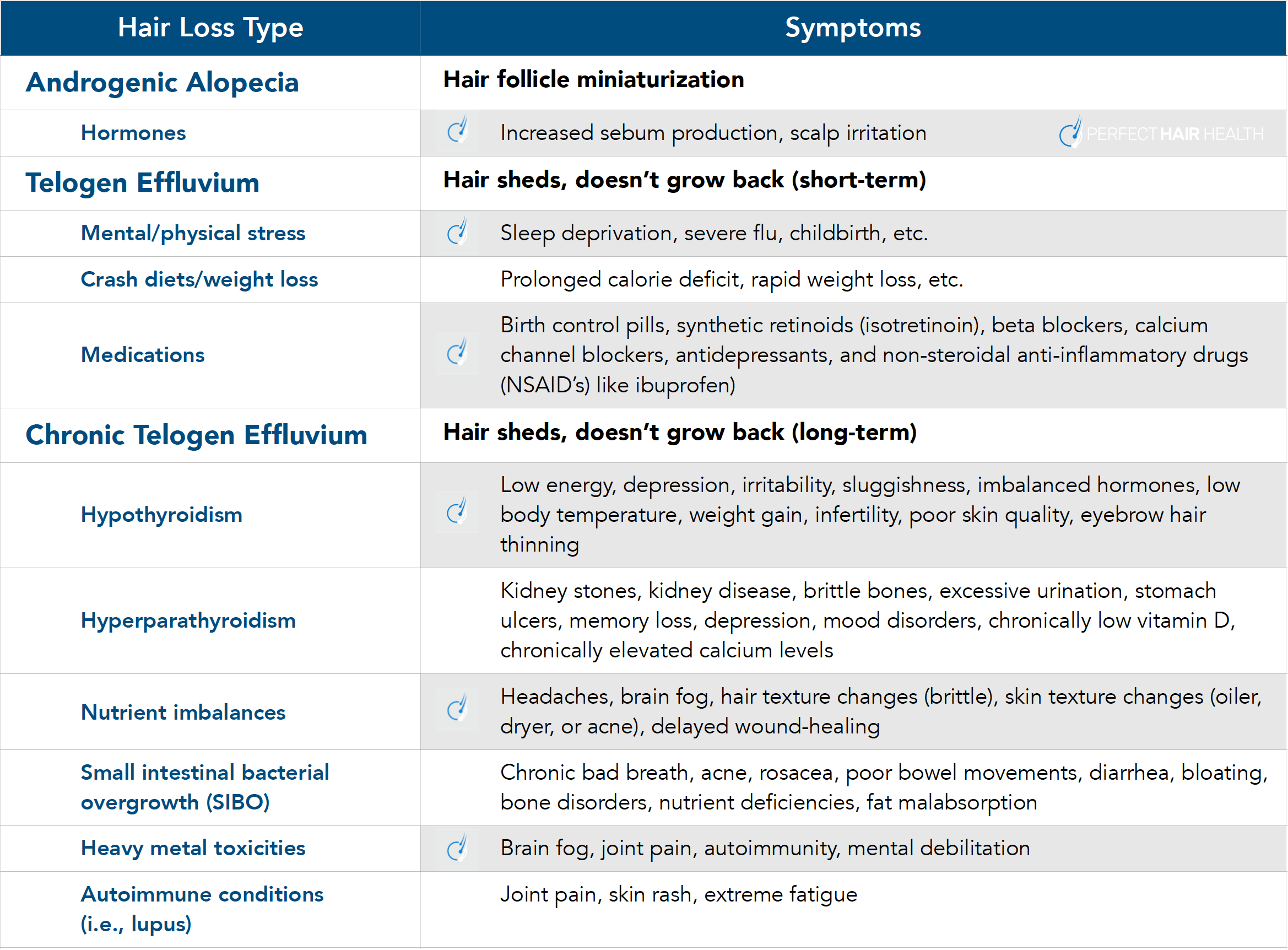
Take that list, and start using it to your advantage! And keep in mind that a huge percentage of hair loss sufferers have multiple forms of hair loss. So, if you fall into multiple categories, that’s okay. You’re just identifying your own potential causes, so can seek more robust treatment options.
The power of identifying your hair loss causes (reader case study)
Here’s a reader case study of someone with whom I’ve worked for years: Ben M.
Ben M. is a male who began experiencing diffuse hair loss in his early twenties. In his first attempts to treat his hair loss, Ben M. only followed treatments for androgenic alopecia – which he’d initially suspected was a problem for him. They only worked to slow or stop his hair loss – if that.
A deeper analysis into his diet, lifestyle, stress levels, and environment revealed that Ben M. was also likely dealing with a hair shedding disorder – specifically, telogen effluvium related to a variety of causes (stress and nutrient deficiencies). So, we began to tackle those causes in addition to continuing to pursue interventions for AGA.
Six months later, Ben M. recovered nearly all of the hair that he’d lost.

If you’re curious to see his photos and full case study write-up, you can do so here.
Note: these results happened only after Ben took the time to evaluate his hair loss presentation alongside his health history, identify additional underlying causes, and then take a multifactorial approach to resolving his hair loss.
Once he targeted all of the underlying causes to his hair thinning, his regrowth skyrocketed. And according to him, it’s remained ever since we worked together.
The bottom line? Identify first, treat second
If you’re dealing with hair loss in a diffuse pattern, it pays dividends to systematically identify which causes of diffuse thinning relate to you. Then, you can prioritize testing for these contributors, and in doing so, fast-track yourself to better hair recovery.
Questions? Comments? Please reach out in the comments section below.

Rob English is a researcher, medical editor, and the founder of perfecthairhealth.com. He acts as a peer reviewer for scholarly journals and has published five peer-reviewed papers on androgenic alopecia. He writes regularly about the science behind hair loss (and hair growth). Feel free to browse his long-form articles and publications throughout this site.
Will this work for seniors as I’m 69 and have had hair loss since my thirties.
It all depends! I’ve worked with many women who’ve started experiencing hair loss between the ages of 30-60, and through a variety of causes (polycystic ovarian syndrome, nutrient deficiencies, female pattern hair loss post-menopause, etc.). In general, I’ve found that the absolute best approach is for someone to prioritize (1) identifying the causes of their hair loss, and then (2) taking steps toward resolving them. With this approach, hair loss can often be improved at any age.
Best,
Rob
Hi Rob, thanks for another great article.
I’ve been a chronic shedder for ~3years now (I’m 24) with almost 70% of my hair gone /: done all the possible lab tests I can, have corrected what needs to be corrected, have no SIBO symptoms at all, but seems like nothing is helping. I do have low temperature and low pulse so I seem to be slightly hypo.
But I was wondering if you’ve come across anyone with thalassemia trait? It’s characterized by very high red blood cell count, but very low mean corpuscular volume and width. It’s not the serious type with no symptoms except sometimes mild anemia.
Can’t help wonder if there’s a link. Furthest I could figure is that all types of thalassemias tend to have lower cholesterol (which I do), and low cholesterol means it’s not being converted to protective steroids. But I’m not sure what’s causing my hypothyroid state.
Appreciate all you do!
Many thanks indeed, Rob. I feel there is hope now for me to conquer my hair loss issue which has seemed like a losing battle for me over these 8 years. You talk a lot of sense and cut through the dross on hair loss. Your honesty and desire to help hair loss sufferers shines through.
Seems I may have hair miniaturisation and anxious to resolve this as my image ie visual hair thinning is making me depressed. I am a ´young ´ 67 female who has been throwing vitamins, MSM, marine collagen etc at my hair loss problem with no real improvement and panicking. A HUGE thank you from me. Linda
Thanks for the kind words, Linda! And I’m sorry you’ve hit so many dead-ends while trying to tackle your hair loss. Please keep in touch, and let me know if there’s anything else I can help with.
Best,
Rob
P.S. – I’d recommend reading a few of our articles about vitamins and their connection (or lack thereof) to most forms of hair loss in the developed world. Here are a few that come to mind – particularly about Nutrafol, vitamin A, and biotin:
https://perfecthairhealth.com/nutrafol-review/
https://perfecthairhealth.com/vitamin-a-retinol-beta-carotene-hair-loss/
https://perfecthairhealth.com/biotin-for-hair-loss/
We also have a product review about Viviscal® inside our membership community (I’m assuming that might be marine protein-based supplement you’re trying).
Best,
Rob
Rob,
my opinion is that hair fall is simply a result of problems in communication among cells. The information theory of aging of professor David Sinclair tells it all. Scalp massages, complex vitamins, DHT suppressants, PRP procedures etc. mean just treating the consequences. I personally had a DHT operation performed in October last year on my temples and treated areas (zero hairs on them then) have now about 2/3 of the thickness of my other parts of the head. I put each morning topical 5% Minoxidil and quit Fin in pills. Implanted hairs are a bit more coarse and the direction of growth slightly differs the other hairs. I just started taking NMN and trans resveratrol as anti aging supplements and do believe they will help keeping my hair in a better state. I am 52 now and am 1B on Norwood scale.
Hey Nikolay,
It’s certainly possible! On the note of cellular cross-talk, you might find these articles interesting…
https://perfecthairhealth.com/scalp-tension-hair-loss/
https://perfecthairhealth.com/hair-transplants-debunk-scalp-tension-hair-loss/
…particularly the last article, where we talk about a mouse study demonstrating paracrine signaling across far distances (i.e., distant hair follicles) for plucked versus unplucked hair follicle tissues.
Would you mind clarifying what a “DHT operation” is? Congratulations on your regrowth so far!
Best,
Rob
Have you heard of any potential causes of thinning behind the ears and around the sideburns? Some say it’s a sign of aggressive MPB on the horizon, while others say possible non-androgenic causes. But I notice that men and women get this, not just aggressively balding men, which makes me unsure of the the former argument.
Very interesting article btw. I’m sure a lot of people suffering with hairloss have a combination of AGA and other contributing issues at play without realising it. But it’s frustratingly difficult to get to the bottom of the problem though, especially if you also have some signs of pattern baldness too.
Hey Josh,
Thanks for reaching out. Loss behind the ears and nape of neck is often associated with pattern hair loss. Having said that, you’re right that this sort of loss isn’t always directly connected to androgens. And interestingly, in women, loss here has been recorded, as miniaturization, and as the classification of female pattern hair loss… even in the complete absence of androgens. So there’s certainly more we need to learn.
This article might interest you: https://perfecthairhealth.com/androgenic-alopecia-aga-characteristics-causes-unknowns/
Some common causes of loss here (that aren’t related to AGA) are the ones listed in this article, alongside certain forms of autoimmune-related hair loss (specifically, ophiasis alopecia areata).
Thank you Rob for a great article. I have been struggling with ridiculous chronic shedding for over 4 years now! I have Kaiser insurance which has been useless in helping me try to get a handle on my hair loss. I have done some testing on my own, but struggle as to how to make sense of it all. I spend so much time on the internet but just wind up more confused and frustrated then the day before. I’ve tried a couple different diets and am at the point that I second guess anything I put in my mouth. I am going crazy! I guess I’m wondering if you (or if you know of anyone else) work with people to help them one on one? I am desperate for help!
Hey Andrea,
Thanks for reaching out. Yes, I do work one-on-one with people inside our membership, and through our Consultation Package. You can learn more here:
https://perfecthairhealth.com/join-now/
The Consultation Package comes with a 60-minute Skype call – where we video chat for an hour to go through your entire health + hair loss history. So that’s the best option if you’re looking for individualized support.
All my best,
Rob
Thanks for the articles as always. A couple questions.
1) With diffuse thinning, is it the entire scalp including sides and nape? I have not noticed normal signs of mpb but definitely have noticed thinning on the entire top of my head especially compared to my nape and sides. Also the hair on my nape and sides is very curly while hair on top is wavy-curly.
2) i am a few months into the daily 2×20 Min massages and havnt noticed any changes yet. Gonna keep pushing fo 8-12 months. But I was wondering how micro needling compares to the massages and if it’s something you think I should add in?
Hey Andrew,
(1) If the diffuse thinning is related to male pattern hair loss, the thinning tends to generally just affect the top of the scalp. If it’s related to female pattern hair loss, it’s often a coin toss between only the top versus all of of the scalp.
(2) In general, most people start reporting positive results with the massages after 6+ months. So, 8-12 months is a great timeframe to evaluate results! Microneedling does carry some mechanistic overlap with massaging – particularly with acute inflammation generation. But there’s certain things that microneedling does better, and there’s certain things that massaging does that microneedling cannot do at all. Inside our membership, we’ve got a lot of information on how to best combine microneedling and massaging (if that’s something you’re interested in trying). The key is to find a balance point between both interventions as to (1) avoid over-inflammation the scalp, and (2) maximize each therapy’s effect.
Hi Rob,
I experience hair shedding from entire body, i.e., moustache, body hair, eye brows etc. But not in patches or like Universalis. Messaging does help on scalp but can’t do that everywhere. Is it a part of AGA or telogen effluvium? What could be the underlying causes?
I eagerly wait for a reply
Thanks!
Hey Devansh,
That sounds less like androgenic alopecia, and more like telogen effluvium and/or autoimmune-based hair loss. With AGA, typically men experience scalp hair loss alongside more body hair growth.
Best,
Rob
Hey Rob, sorry, my post was sent before I had finished editing it. 🙂 Here’s what it should have said. 🙂
I’m Garrett Lambert. I am a 71 year young man and my hair was starting to recede in 1994 and I met a guy named Anthony Morrocco who became a close friend. He was just beginning to create a company called the MorroccoMethod.com And it was all about eating organic and healthy, using his holistically balanced on based on the 4 elements, using them along side Raw Organic Apple Cider Vinegar with the Mother, He taught me about getting your hair cut on the Lunar Cycle and getting a blunt acupuncture/acupressure type of cut that he learned while traveling to Brazil and China. He talked to me about brushing my hair 50 to 100 times, 2 times a day and it seemingly miraculously started growing back and continued to do so until about six or seven years later in 2001 when I started taking testosterone inducing products and was put on testosterone gel because of Low testosterone levels. And it continued to slowly recede from 2001 to about 2015 and then I had a stroke and was put on Xarelto and then Eliquis and Crestor and noticed that it began to recede even faster
I was also simultaneously taking and using many of the things that were recommended for hair loss such as a Derma Roller, Finasteride, Dutasteride, Rogaine, different variations of minoxidil 15% ++, etc. etc. And nothing seemed to help. And as I mentioned I had a mild stroke in November 2015 and they put me on blood thinners Xarelto and then recently in the last couple years Eliquis and Crestor. And I noticed my hair receding back more rapidly than ever all cross the front of my scalp and the temple areas.
About 2016 or 2017 I started using a derma roller and ended up causing abrasions on my scalp and subsequently getting scalp psoriasis which exist to this day. It was scaly and inflamed all over my head until about a year or so ago when I started brushing it less harshly and etc. It’s still definitely inflamed but not to the point of being scaly and extremely irritated at least on my forehead. etc.
Rob I’m wondering if the scalp psoriasis in combination with the blood thinners have just exacerbated it. I brush my hair 50-100 times 2 X a day, take Collagen protein, Niacin and it’s still receding so extraordinarily quickly, it’s shocking. I get almost 2 handfuls of hair when I brush my hair and also when I wash it. I use 2% Ketaconazole Shampoo which I combine with Alpecin Caffeine Shampoo.
It’s just unbelievable how quickly my hair has receded all across the front of my scalp and back on both sides over 2-3 inches over the last year or so and has really accelerated in my view over the last year. My health is seemingly great, blood pressure and pulse rate on the low side, 5’9′ about 145 lbs. I’ve been jogging for over 50 yers, eat organic healthy food, don’t smoke or drink, meditate and love God, my Beloved woman, my family, friends and life!
I’ve been to many dermatologist and they say the usual things. I’m not sure what else to do other than get PRP and stem cells, or hair transplant, I was even thinking about getting a Grow band by Hairguard.com or a lazer band, etc. I’d love to get any of your thoughts and input my brother, thank you Rob. Sending Rich Blessings, Garrett Lambert
Hey Garrett,
Thank you for the kind words, and thanks for reaching out.
I’ve read through your full comment. Given the level of detail, the specificity of the questions, and the number of things to discuss, this type of conversation is better suited as a Skype Consultation (which can be booked through our membership community).
In the meantime, my directional advice would be to hold off on any more product purchases (i.e., Growband, stem cells, hair transplant, laser helmets, etc.) until you’ve got some better direction as to what might be contributing to your thinning. It seems like there may be a drug interaction and some degree of autoimmunity (as evidenced by the scalp psoriasis). At the same time, I’d need to learn more about your story and health history before being able to better comment.
All my best,
Rob
Hi Rob! Thanks again for this great article. I wish there were doctors who read this too :).
I had a question i hoped you could help: what i notice at my hair ( besides loosing them) is that while the hair itself looks the same ( not thinner) the point of it is very thin(like sth that has no nutrition to grow). Does that mean a hair follicle miniaturized??
I also just checked for thyroid and T3 was at minimum level of the range(1 compared to minimum level of 0.92) _ if that is of any relevance. I would really appreciate yr opinion on that. Many thanks,
Holta
Hey Holta,
Thanks for reaching out. Based on what you’ve described, this sounds a bit like alopecia areata. Have you ever looked up photos of the “exclamation point” hairs found in cases of diffuse alopecia areata? This is a relatively rare type of hair loss, but it might have overlap with what you’re describing.
If possible, I’d try to connect with a dermatologist to see if they can better describe / diagnose what is going on.
Best,
Rob
Nice article Rob. I’ve interacted with you over the years and exchanged emails, and I am happy to see you being so successful. I bought your book back in 2016, and I still enjoy reading it from time to time, it was very well done.
You cited some very nice sources and it’s well written as usual. I don’t agree with you that there is such a thing as AGA. I think the hair follicles miniaturize when they’re continuously exposed to cortisol and elevated prolactin, chronic tension etc. From my point of view the genes or androgens don’t have anything to do with it. But it’s fine if we disagree, that’s totally normal.
I keep wishing Danny Roddy would invite you on his YouTube bioenergetics streams. Yes you have diverging points of views, but I think that’s the interesting and most beautiful aspect of human interactions, the ability to disagree and still be respectful and have a discussion.
Congrats on your work, and hope you’re well!
David B.
Hey David,
It’s great to hear from you. Thank you for continuing to read our articles, and for your support to keep the site running.
I’ve always found Danny Roddy to be incredibly respectful, well spoken, and in general, a really nice guy who prioritizes helping people above all else. I believe we disagree on aspects of the pathology of certain hair loss disorders. At the same time, I’m sure there are aspects of his arguments that I either misunderstand or don’t fully understand. I’m always open to learning and conversing with others with a different point of view.
I hope all is well with you and your family during these crazy times.
All my best,
Rob
Interesting read. I had a thinning hair for 8 years now, started with excessive shedding I didn’t pay much attention to because the lack of growth wasn’t noticeable for a long while. 5 years in I was diagnosed with hyperparathyroid adenoma which I also had for a few years – my calcium was through the roof and at the moment my mental state was quite deteriorated (piling on my initial stress from the hairloss itself). After a successful surgery I felt reborn the very next day and my hair shedding stopped… for like a two weeks. Now it’s still going on, and the thinned region of my scalp takes a triangular pattern – from top of the skull towards the temples (and right side is visibly thicker for some reason). Massaging for about 10 months by your 2nd edition method didn’t bring any progress except for loads of dandruff for which I had to start using a nizoral shampoo. Guess now I’ll have to look into bacterial overgrowth you’re talking about. I don’t have much hope left since my father’s head was shiny like a fortune teller’s ball in his early 30s, but losing hair would still suck.
Hey Rob, 8 years ago I started scalp massage 2 X 20 minutes each day and after persisting for 2 years the bald patch on my crown recovered about 40% of the hair I lost. 19 months ago a dermatologist found I had melanoma so I improved my diet, exercise routines and optimum sunshine for Vitamin D. My skin cancer has now disappeared but during the same period I lost most of the hair on my crown again despite daily scalp massaging. I am now 65 and I assume age counts against me now despite everything I have been doing for healthy hair and skin.
Thanks for another great article, after all these months of struggle, I found AGA to be the easiest one to deal with, I can stop hairloss and regrow my receding hairline and temples simply by daily scalp massage and weekly dermarolling, but I also have diffuse thinning, I think it has something to do with fatigue, I started experience very aggressive shedding since I gained much weight, although I’ve stopped shedding through diet & lifestyle changes and also scalp massages, but the hair on my crown area still grow very slowly. Now I decide to exercise more to get a healthy body and lose more weight. Wish I can succeed.
Hi Rob, thanks for the information. Like Devansh, I was losing hair all over my body and I started following the advice of More Plates More Dates. My scalp hair loss is in a diffuse pattern on the top and sides, kind of similar to Ben M. I am cautious about side effects so chose the methods with the least sides. So I used Nizoral 1 or 2 times a week for a year but it didn’t make much difference apart from getting rid of my dandruff. I’ve been using oral castor oil 1/2ml a day for 6 months now and its great for regrowing hair, it has brought my body hair back to normal now but I’m still losing my scalp hair in a diffuse pattern, the hairs I have do appear thicker and it does look like I’m growing some hair back. In addition to this, for the last 9 weeks I’ve been doing micro-needling once a week, another thing has appears to be growing some hair back or making them thicker but not stopped my hair loss. I count the hairs I lose in the shower everyday and its been consistent (and slightly growing since lockdown started).
In terms of your causes/symptoms table, I do have minor scalp irritation maybe once or twice a week. I do think I am long term sleep deprived and get 6 or less than 6 hours of sleep most days. My weight loss regime is long term calorie deficit (50-100 calories less than what I use) and I also weight train 5 days a week, so my diet is mainly protein based. I don’t take any medication but I do take Cod Liver Oil and Glucosamine Chondroitin & MSM Complex Liquid (joint health). I do feel sluggish most days and low energy/tired. I’m not sure if I’m low on Vit D but I think the Cod Liver Oil covers that? I very rarely get headaches and never get brain fog. I do have some body acne too.
Any advice would be recommended. My research and also reading the Ben M Case Study indicates that I should get more sunlight (I guess supplements aren’t as good) and sleep more. Sleep deprivation raises cortisol levels which can reduce thyroid function, so in that way it makes sense.
Hey Rob!
Thanks for the amazing article. I am suffering from diffuse thinning since the age of 14 and it has slowly gotten thinner over the years. Of course, I am not able to tell if AGA plays an important role in my case. Since childhood, I have always had dry skin, nail problems, skin lesions (acne entire body), and digestive issues. A few years later I made a lab test and found out that I was very deficient in Zinc (active athlete as well). After I started supplementing with Zinc (40mg) and eating more zinc-rich foods (beef, chicken liver, canned oyster) almost after a day, my digestive issues faded and now I am 4 months in (+ daily 30 min massage). The hair count itself has not changed but my hair is a lot darker then it was four months ago and will see how things might improve. Sorry for the long message but here are my questions:
-do you think it is ok to eat around 400g of chicken liver on a weekly basis? I don’t really think that it could have an overdosing effect of Vitamin A (retinol), and have a negative influence on my hair growth regimen.
-with all the things I have mentioned and additionally a healthy balanced diet (eating liver, beef, fish, oyster, a lot of raw green vegetable, fruits potatoe, rice, banana as a staple), everyday sun exposure, active lifestyle, weekly derma rolling and no shampoo: would it still be ok to use topical minoxidil as a bonus? Or do you think that the 95% alcohol might have negative effects on my scalp? (of course, our scalps would react differently but in general, would you rate minoxidil as a positive extra?)
Hope you have time to answer.
Hello Rob,
I’d like to begin the massage regimen for my follicle miniaturization. An issue I have however is that I have pretty severe arthritis, particularly in one hand. I can’t imagine being able to massage my scalp for 20 minutes. Would it be effective to do four 5 minute massages throughout the day? Thanks!
Hello Rob,
Wonderful write up. I must say your article explains so much. Thank you for it.
However, I would like to get your opinion on my experience. I am 33 years old, and most recently I have moved to the UK from Singapore for the first time in my life. I have had hair loss for the past 5 years however it wasn’t really obvious, it was receding on the temples and slightly thinning at the top. However, I’ve noticed my hair shedding at a very rapid rate once I moved to the UK. Could the weather and the water have accelerated my hair loss?
Thank you
hi rob
My hair follicles are becoming smaller. But hair loss progresses slowly. I have been taking finasteride for more than a year. Also has been taking vitamin zinc and so on. There was no significant improvement. What do you think may be my reason?
Hey Rob. Have you ever heard the thoughts on wearing hats/cap contributes to hair loss? What are your insights about this? Is it a fact or just a myth?
I think it can act as an accelerator of hair loss via pressure alopecia, but only through very specific circumstances – for instance, really tight hats worn for multiple hours with little (if any) movement or breaks while wearing the hat. For most usage parameters, I think hats are not contributive!
Hi Rob, Ayush this side from India. I love watching your videos as they are very informative and straight to the point. I am 20 years old and have been experiencing diffused pattern of hair loss since I was 17. I met my dermatologist and he prescribed me Minoxidil 5% and gave me a Ketoconazole shampoo. I have been using minoxidil for 7 months now but haven’t got any significant results yet, I think that I am not a good responder to minoxidil. I have also been doing daily scalp massages of 15 minutes for 3 months after seeing some of your videos, hopefully it’ll bring some good results in the future.
From last 3-4 weeks, I am experiencing increase in my hair fall. I used to shed around 15-20 hairs daily but now I am shedding about 100-110 hairs daily and 80-85% of these hairs are very thin and some of them are so thin that it becomes very difficult to see through naked eyes. I think that I am still loosing them. I visited my dermatologist and told him about this situation and asked whether I can use finasteride but he denied and told me that I am too young to use it. I doubt that I’ll lose most of my hairs till I’ll become eligible to take finasteride as minoxidil is not helping in retaining the hairs that I have currently. Plzz help me out.
Thanks for the kind words, Ayush!
Right now, in the Northern Hemisphere, we’re experiencing a period of increased shedding due to seasonality. This tends to peak in July and August. So, perhaps some of your recent shedding could be attributed to this.
Otherwise, the shedding might be related to the advancement of AGA. Technically speaking, since you are 20 years old, you are qualified for a prescription of finasteride. If that’s something you want to try, another dermatologist should be able to prescribe it to you. To mitigate the risk of side effects, you can always start with topical and see how you respond. Perhaps your dermatologist would be more likely to start you with a topical formulation first.
Best,
Rob